Contemporary Research Into Neurological Disorders (VCE SSCE Psychology): Revision Notes
Contemporary Research Into Neurological Disorders
Introduction to neurological disorders
Neurological disorders encompass any condition affecting the nervous system, including the brain, spinal cord or peripheral nerves. With over 600 different types identified, these conditions represent a major health challenge globally.
These disorders can develop through various pathways. Some result from acquired brain injury (ABI), while others are congenital conditions that develop during foetal development. Throughout life, the nervous system remains vulnerable to damage from trauma, nutritional deficiencies, substance use, infections, and various diseases.
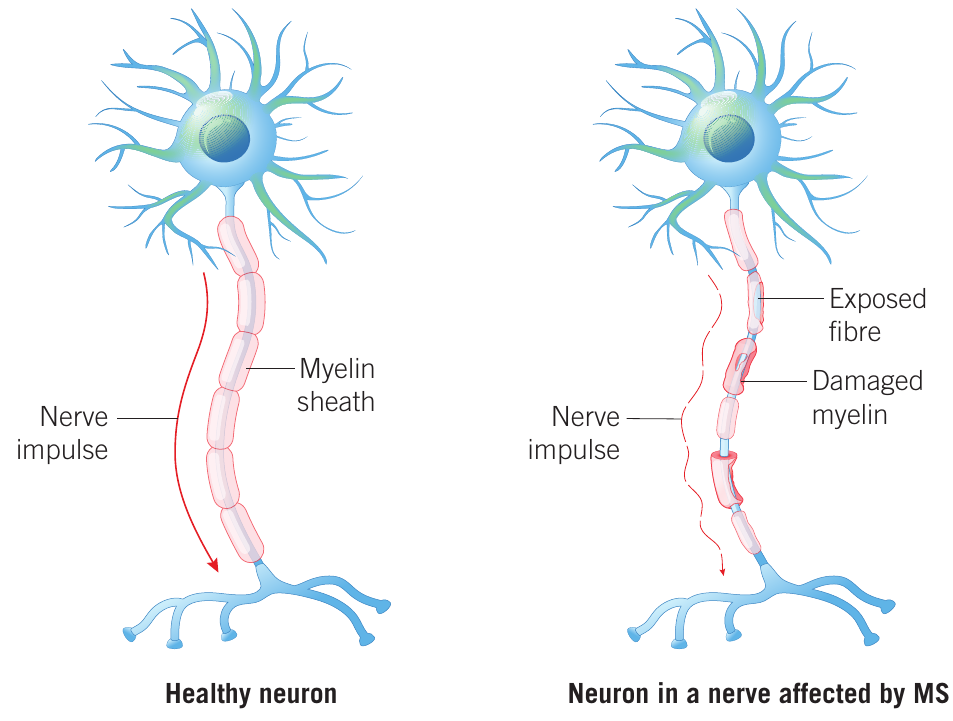
The impact of neurological disorders is typically long-lasting and can affect multiple aspects of functioning, including language, movement, vision and cognition. Poor mental wellbeing commonly accompanies these conditions. Examples include dementia, cerebral palsy, meningitis, motor neurone disease, migraines, epilepsy, multiple sclerosis and Parkinson's disease.
As populations grow and age globally, neurological disorders are becoming an increasingly prominent cause of death and disability. This trend underscores the importance of ongoing research to develop better understanding, treatments and potential cures for these conditions.
Epilepsy
Understanding epilepsy
Epilepsy is a neurological disorder characterized by sudden, intense bursts of abnormal brain activity that result in seizures. These are recurrent and unprovoked episodes, distinct from seizures caused by temporary conditions such as high fever, blood sugar fluctuations, substance withdrawal or concussion.
During normal brain function, neurons fire in an orderly sequence as messages pass through the brain. In epilepsy, this pattern is disrupted. Seizures occur when excessive numbers of neurons fire synchronously, creating abnormal electrical activity throughout affected brain regions.
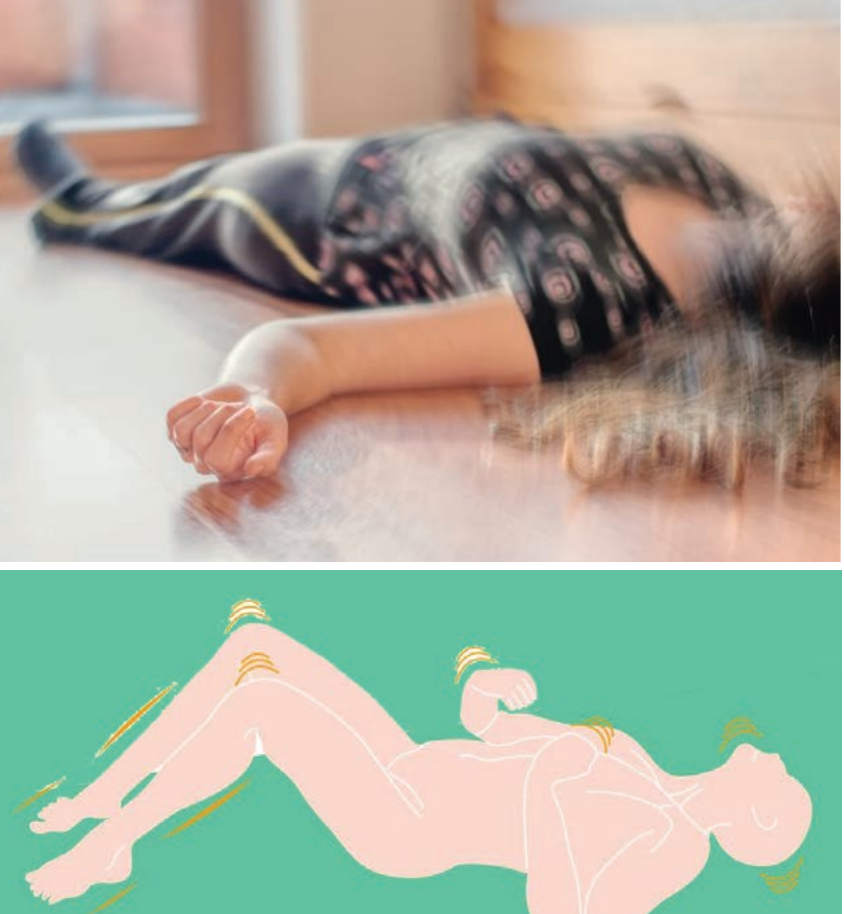
Key term: A seizure is an uncontrolled rapid movement or shaking of body parts (also called convulsions), usually accompanied by loss of awareness or unconsciousness.
Causes of epilepsy
Epilepsy affects approximately 1% of the Australian population and is most common in young children and older adults. In many cases, the cause remains unknown. However, identified causes include:
- Brain tumours
- Improperly formed blood vessels
- Serious head injuries
- Stroke
- Brain infections
- Alzheimer's disease
- Loss of oxygen at birth
- Hardening of the arteries
- Genetic factors
Some mild forms appearing in childhood may resolve before adulthood without treatment.
Following brain injury, early seizures may occur within days to weeks due to bleeding, trauma or swelling. These often resolve as the initial injury heals. However, later-onset seizures may result from brain scarring, causing cells to malfunction. In such cases, epilepsy may be diagnosed.
Types and symptoms of seizures
Various epilepsy syndromes exist, including Rett syndrome, Rasmussen's syndrome and juvenile absence epilepsy. Seizures fall into three main categories based on how much of the brain is affected:
Generalised onset seizures
These affect both brain hemispheres simultaneously. Symptoms include:
- Sustained rhythmic jerking movements
- Muscles becoming weak, limp, tense or rigid
- Repeated body flexing and extending
- Staring and making noises
- Falling down
- Loss of consciousness
- Confusion and tiredness upon regaining consciousness
- Breathing cessation
- Loss of bladder control
- Tongue biting
Focal onset seizures
These begin in one specific brain area on one side and affect particular body parts depending on seizure location. Symptoms include:
- Jerky or rhythmic movements
- Tense or rigid muscles
- Brief muscle twitching
- Lack of movement
- Repeated automatic movements (clapping, running, chewing)
- Tingling and dizziness
- Staring and confusion
- Changes in emotions
- Altered sensations
Some individuals experience warning signs (auras) before focal seizures, including feelings of déjà vu, impending doom, euphoria, or visual/hearing changes.
Unknown onset seizures
These occur when the beginning is not observed and may later be reclassified as generalised or focal.
Risks associated with epilepsy
Whilst seizures themselves rarely cause death directly, they present several serious risks.
Critical Safety Considerations:
Long convulsive seizures lasting over five minutes constitute a medical emergency and can be fatal. Additionally, seizures occurring during dangerous activities (driving, swimming) can lead to accidents. Falls during seizures may cause broken bones or head injuries.
From a psychosocial perspective, epilepsy can strain relationships and limit work and recreational activities. The stigma and discrimination surrounding epilepsy often concern individuals more than the seizures themselves.
Diagnosis
Epilepsy diagnosis involves several approaches:
Electroencephalograph (EEG)
An EEG detects, amplifies and records the brain's electrical activity. Electrodes placed on the scalp can identify unusual spikes or waves in brain activity patterns, aiding diagnosis based on epilepsy type.
Brain imaging
MRI (magnetic resonance imaging) and CT (computerised tomography) scans can identify affected brain locations and detect scar tissue, tumours or other structural abnormalities causing seizures.
Treatment options
Treatment is tailored to the type, frequency and severity of seizures, along with the individual's age, health and medical history.
Medication
For most people with epilepsy, anti-seizure medication can reduce seizure frequency or prevent them entirely. Some individuals may never experience another seizure. Finding the most effective medication may require trialling different options. People can also learn to identify and avoid personal seizure triggers.
Surgical interventions
When medication proves ineffective, several surgical options exist:
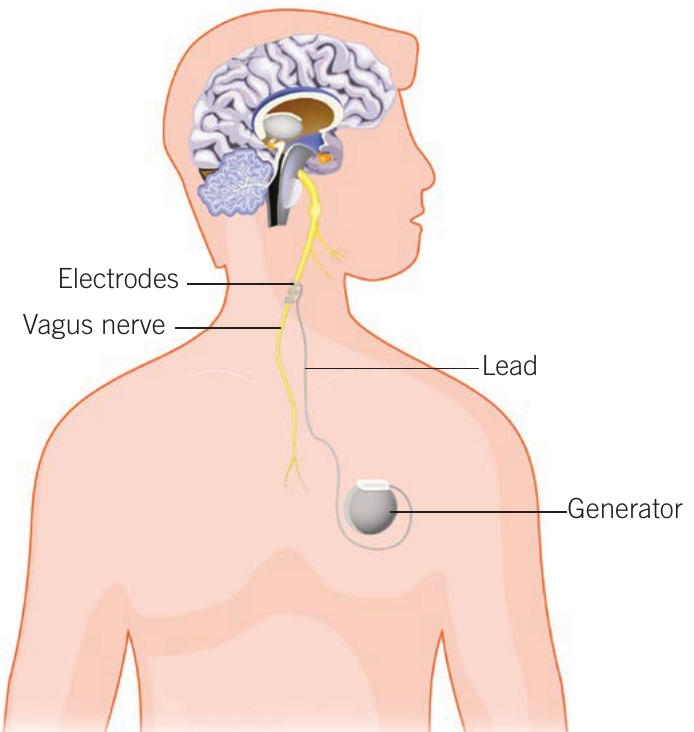
Vagus nerve stimulation
This involves implanting a device under the chest skin that sends regular, mild electrical impulses to the brain via the vagus nerve in the neck. A pulse generator connects to the vagus nerve through thin wires. The device automatically delivers programmed stimulation at specific intervals (e.g., 30 seconds on, 3 minutes off).
How Vagus Nerve Stimulation Works:
These impulses may control seizures by:
- Modifying brain activity
- Stimulating blood flow
- Raising neurotransmitter levels
- Modulating nerve pathways involved in seizures
Individuals can also use a handheld magnet to trigger extra stimulation if they feel a seizure approaching.
Other surgical implants
Deep brain stimulation and responsive neurostimulation work similarly, detecting seizure activity and delivering electrical stimulation to prevent or stop it.
Tissue removal
For severe cases where seizures consistently originate in one brain area, that specific region may be surgically removed to prevent the spread of abnormal electrical activity. This approach is only viable when the affected area is not involved in critical functions like speech, movement, memory or vision. Structural abnormalities such as tumours or abnormal blood vessel clusters can also be removed surgically.
Advanced techniques include MRI-guided laser ablation or radiation, which can remove tissue (such as scar tissue) without opening the skull. In extreme cases, the corpus callosum connecting the brain's hemispheres, or even an entire hemisphere, may be removed.
Emerging epilepsy research
Current and emerging research aims to improve outcomes for people with epilepsy. Exciting developments include:
- New drug formulations
- Wearable or implantable technology to detect seizures or falls
- Advances in vagus nerve stimulation, laser ablation, EEG, MRI and ultrasound
- Implantable cooling devices
- Better understanding of ketogenic diets, gene therapy and cannabinoids
- Improved diagnostic tests, fall safety equipment and seizure prediction algorithms
Chronic traumatic encephalopathy (CTE)
History and definition
Chronic traumatic encephalopathy (CTE) is a neurodegenerative disease linked to repeated head impacts. It was first identified in 1928 by Dr Harrison Martland as "punch drunk syndrome" through a small case study of boxers. These athletes experienced various cognitive impairments and developed a severe, progressive syndrome including Parkinson's disease and dementia.

As more cases emerged, the condition acquired various names, including "traumatic progressive encephalopathy" and "dementia pugilistica". From the 1940s onwards, "chronic traumatic encephalopathy" became the accepted term, acknowledging that the condition arises not only from boxing but from various sources involving brain trauma.
CTE is most commonly observed in athletes from high-contact sports who have experienced multiple head impacts (with or without concussion). These sports include American and Australian football, ice hockey, boxing, rugby, soccer, wrestling, basketball and baseball. CTE also affects military personnel who have experienced blast impacts, domestic violence survivors, and individuals with self-injury from head-banging behaviours.
Physiological basis of CTE
As a neurodegenerative disease, CTE causes gradual, progressive and widespread brain damage. The key pathological feature involves the accumulation of tau protein within neurons and other brain cells.
Understanding Tau Protein:
Tau protein is normally required by cells for stability. In a healthy brain, excess tau is broken down and removed as part of normal functioning. In CTE, this process malfunctions. Whilst the exact mechanism remains poorly understood, repetitive head injuries appear to trigger tau aggregation, which then accumulates and spreads with age.
The accumulated tau disrupts important cellular processes that keep cells alive and healthy, and interferes with communication between adjacent neurons. This compromises brain tissue integrity and begins killing neurons and other cells, resulting in widespread atrophy of many brain regions and reduced brain volume.
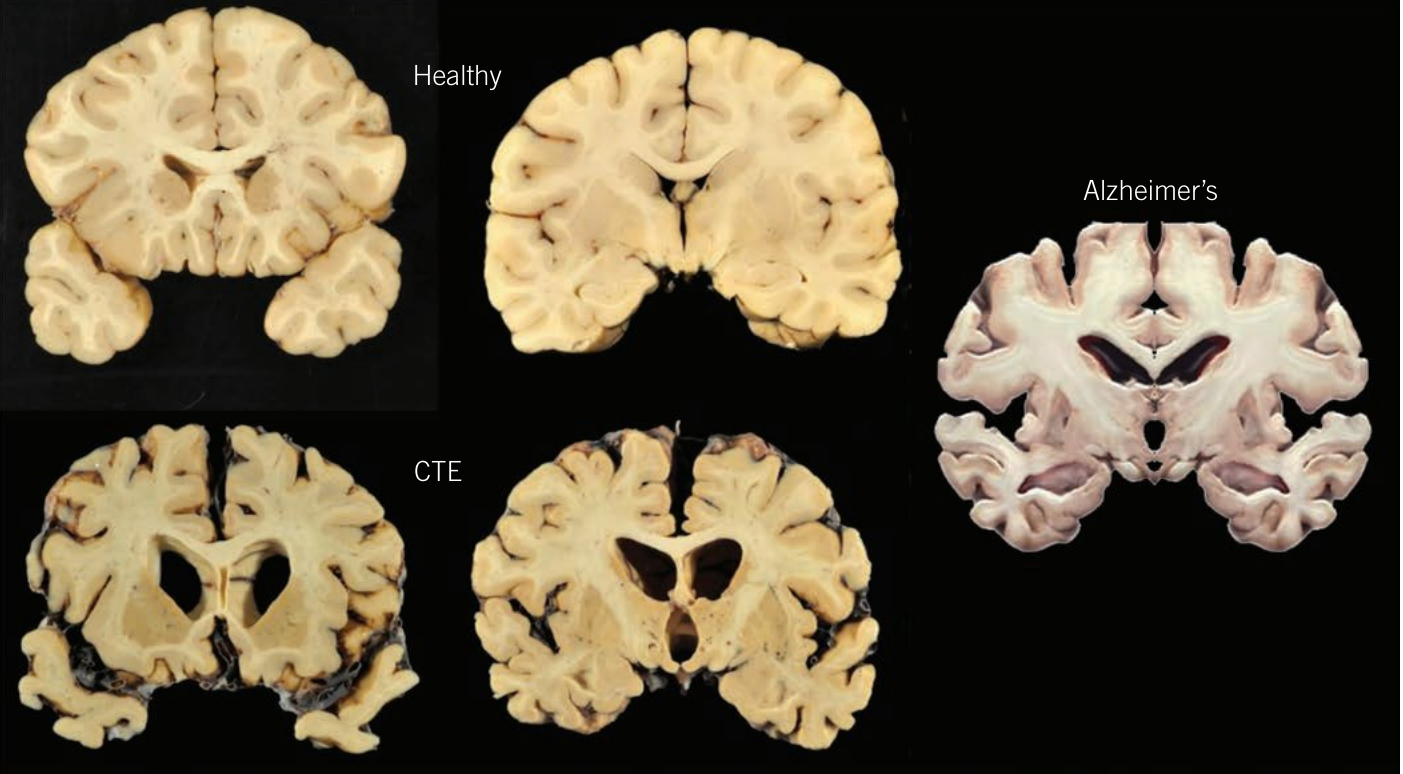
CTE is often mistaken for Alzheimer's disease because both conditions involve tau protein accumulation. The brain changes in CTE and Alzheimer's disease are physically similar, as shown in the comparison of brain tissue cross-sections above.
Causes and risk factors
Whilst not every concussion or traumatic brain injury leads to CTE, such head injuries appear necessary to trigger the disease. The precise amount of trauma required remains unknown, but those experiencing increased head impacts face greatest risk. All blows to the head, whether causing concussion or not, likely contribute to disease development.
Additional Risk Factors:
Besides the number of impacts, other possible risk factors include:
- Timing of injuries
- Location of impacts
- Severity of injuries
- Genetic factors
- Lifestyle factors
Symptoms and stages
CTE worsens progressively over many years. Research has identified four main stages, demonstrating declining function as the disease progresses. Early symptoms become more severe over time, and new symptoms emerge. These stages correlate with increasing tau protein pathology and subsequent brain tissue degeneration.
The Four Stages of CTE Progression:
Stage 1
- Headaches
- Inattention and poor concentration
- Mild aggression and explosivity
- Mild memory dysfunction
- Mild depressive symptoms
- Finite number of isolated tau protein clusters in specific brain areas
Stage 2
- Increased cognitive and memory dysfunction
- Behavioural changes
- Increased aggression and explosivity
- Increased depression
- Suicidality
- Multiple clusters of tau protein
Stage 3
- Further increased cognitive and memory dysfunction
- Mild dementia
- Executive dysfunction (difficulty planning, problem-solving, organizing, managing time)
- Further increased aggression and explosivity
- Further increased depression
- Suicidality
- Moderate tau deposition
- Reduction in brain weight
- Mild brain atrophy
Stage 4
- Severe cognitive and memory dysfunction, including language deficits
- Severe dementia
- Paranoia
- Pervasive aggression and explosivity
- Depression and suicidality
- Motor symptoms, including Parkinson's disease
- Severe tau deposition across most brain regions
- Significant decrease in brain weight
- Profound global brain atrophy due to widespread neuronal loss
Diagnosis challenges
Currently, no conclusive tests can diagnose CTE in living patients due to a lack of distinct biomarkers or measurable indicators. Clear diagnosis is only possible post-mortem during autopsy.
Diagnostic Limitations:
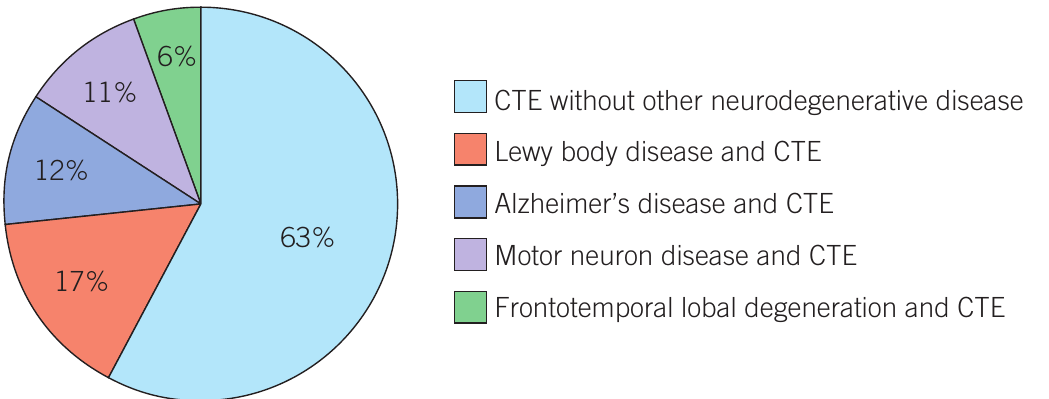
Diagnostic difficulty is compounded by symptom overlap with other neurological disorders, particularly Alzheimer's disease. It is quite common for other neurodegenerative diseases to be diagnosed alongside suspected CTE.
Approximately 63% of CTE cases occur without other neurodegenerative diseases, whilst 37% present with comorbid conditions including Lewy body disease (17%), Alzheimer's disease (12%), motor neuron disease (11%), and frontotemporal lobal degeneration (6%).
The repetitive trauma or tau accumulation in CTE may provoke further abnormal protein development, potentially triggering other neurodegenerative diseases.
Treatment and prevention
Treatment limitations
CTE is currently incurable and irreversible. Similar to other neurodegenerative diseases, treatment focuses on managing symptoms with medications and therapies aimed at improving impaired behavioural and cognitive functioning, such as memory, mood and alertness. Lifestyle habits promoting health and wellbeing are encouraged, including good nutrition, physical activity, and mental and social engagement. Like time-sensitive stroke treatment, timely traumatic brain injury treatment could reduce CTE development risk.
Prevention strategies
Prevention remains the most effective approach to combating CTE. Several strategies have been implemented:
Sports rule changes
Modifications to how contact sports are played, including rules for safe tackles and penalties for reckless play, have helped prevent head injuries. Clear processes are needed to track injuries and symptoms over time.
Worked Example: AFL Concussion Management Protocol
In 2020, the Australian Football League (AFL) introduced stricter concussion management policies. The new rules mandate:
Minimum Recovery Time:
- Medical clearance required at least 5 days before the team's next scheduled competition match
- Effectively requires at least 12 days between experiencing concussion and playing the next match
Six-Stage Graduated Return-to-Sport Protocol:
- Rest: Complete physical and cognitive rest
- Symptom-limited activity: Gradual reintroduction of daily activities
- Light aerobic exercise: Walking or stationary cycling
- Sport-specific exercise: Running drills without head impact
- Non-contact training drills: Progressive resistance training
- Full contact practice: Following medical clearance
- Return to sport: Normal game play
These changes help ensure adequate recovery time before returning to competition safely.

Protective gear considerations
American football helmets protect against skull fractures but may not prevent concussions and CTE. Traumatic brain injury can result from violent brain acceleration and deceleration inside the skull, against which helmets offer no protection.
An unconfirmed theory called risk compensation suggests protective gear may create a false sense of security, causing wearers to take more risks. American football players often lead with their heads in contact, whereas AFL and rugby players without helmets try harder to keep heads out of contact. Better protective gear may be part of the solution, but this complex area requires careful approach.
Emerging CTE research
Given the importance of physical exercise and popularity of contact sports, ongoing CTE research is vital. Much remains to be learned about the disease.

Drug development
Researchers are experimenting with drugs to stop dementia development from repeated head injuries. New drugs may block certain neurotransmitters that cause abnormal tau protein accumulation following head injury. Success in animal models has led to plans for human clinical trials.
Early detection methods
Studies have investigated early detection and quantification of CTE in living patients using neuroimaging techniques. MRI technology advances enable brain volume measurement and white matter abnormality detection associated with CTE. PET (positron emission tomography) neuroimaging may use tracers to bind to and track tau protein. These techniques, alongside genetic testing, may enable early CTE detection.
Diagnostic criteria development
Research aims to develop agreed-upon criteria for diagnosing CTE during life. Consensus is needed regarding necessary features for CTE diagnosis. Proposed criteria require both substantial exposure to repeated head impacts and core clinical features not fully explained by other conditions. Reaching consensus in diagnostic features will help advance research with greater confidence in finding validity and reliability.
Additional research areas
Studies are investigating:
- Biological markers for diagnostic blood tests
- Role of genetics
- Influence of age, playing position and career length
- Environmental risk factors (stress, alcohol, substance abuse)
- Gender equity in sports concussion research
- Research into younger athletes
- White matter and blood vessel damage beyond tau accumulation
The 2020 case of 29-year-old AFLW player Jacinta Barclay highlighted these needs. Post-mortem analysis revealed cerebral white matter degradation unusual for someone so young and physically healthy, emphasizing the importance of research into younger athletes and gender equity in concussion studies. It also shed light on CTE's detrimental effects on mental wellbeing.
Key science skills: presenting data in tables, charts and graphs
When presenting research data, choosing an appropriate format is essential for others to understand findings. The presentation format depends on the data type, as what works for one type may not suit another. In VCE Psychology, you need to use tables, bar charts and line graphs.
Tables
Use when:
- Data cannot be presented in one to two sentences
- Highlighting important data for quick reference
- Showing precise values is more important than showing trends
Bar charts
Use when:
- Showing trends, patterns and relationships is more important than exact values
- Data has discrete (separate) categories
- Visually comparing several categories quickly
- Data has large differences between categories
- May include grouped or stacked data for subsections
Line graphs
Use when:
- Showing trends, patterns and relationships is more important than exact values
- Data is numerical and continuous
- Tracking small changes over time
- The straight line shows how one data point continues to the next
- Can estimate values between points
- Comparing multiple data sets using multiple lines
Worked Example: Choosing the Right Format
Consider data showing percentage of patients with CTE pathology across five sports:
- Football: 78%
- Boxing: 79%
- Ice hockey: 74%
- Rugby: 75%
- Soccer: 61%
As a table: Use when precise values are important
As a bar chart: Use when visual comparison between sports is the priority
Not a line graph: Line graphs are inappropriate here because the data represents discrete categories (different sports) rather than continuous numerical data tracked over time.
Remember!
-
Neurological disorders affect over 600 conditions involving the nervous system, causing long-lasting impacts on various functions and representing a leading cause of death and disability globally.
-
Epilepsy involves abnormal, excessive synchronised neuronal activity causing seizures, classified as generalised, focal or unknown onset, and is treatable through medication, surgical implants like vagus nerve stimulation, or tissue removal procedures.
-
Chronic traumatic encephalopathy (CTE) is a progressive, currently incurable neurodegenerative disease triggered by repeated head impacts, characterized by tau protein accumulation causing widespread brain damage across four increasingly severe stages.
-
CTE diagnosis currently requires post-mortem examination, though emerging research focuses on developing early detection methods, diagnostic criteria, and treatments to reduce tau accumulation and improve outcomes for affected individuals.
-
Prevention remains the most effective approach to CTE, implemented through sports rule changes, graduated return-to-sport protocols (such as the AFL's 12-day minimum recovery period), and careful consideration of protective equipment effectiveness.