Health, Mortality and Morbidity (AQA A-Level Geography): Revision Notes
Health, Mortality and Morbidity
Understanding key concepts
Before exploring patterns of health and disease, it's essential to understand the core terminology used in this topic. These terms help us measure and describe the health status of populations across different regions and time periods.
Health - The World Health Organisation (WHO) defines health as a state of complete physical, mental and social wellbeing. It's not simply the absence of disease or illness. This broader definition recognises that true health encompasses multiple dimensions of human experience.
Mortality - This term refers to death within a population. It can be measured through various rates including death rate, infant mortality rate, child mortality rate and case fatality rate. These measures help us understand patterns of death across different populations and age groups.
Morbidity - This describes the state of being ill or unhealthy with a disease, or the symptoms associated with a disease. Morbidity also refers to the incidence (frequency) of disease within a population. Certain highly infectious diseases must be legally reported, including malaria, rubella and tuberculosis.
Non-communicable disease (NCD) - A medical condition that cannot be transmitted between people. These diseases are non-infectious and include conditions like heart disease (the largest cause of deaths globally), cancer, diabetes and chronic respiratory diseases.
Disability-adjusted life years (DALYs) - A measure that calculates the burden of morbidity in a society. DALYs measure the number of years of healthy life lost due to poor health or disability. This metric helps compare the overall health impact of different diseases and conditions.
Epidemiological transition - The process through which patterns of disease and mortality change over time. This transition typically moves from high infant and child mortality with frequent infectious disease epidemics towards a pattern dominated by chronic degenerative and lifestyle-based diseases.
Well-being refers to the overall state of being comfortable, healthy or happy. It encompasses physical, mental and emotional health.
Determinants of health
Health outcomes are influenced by multiple interconnected factors operating at different levels. The Dahlgren and Whitehead model illustrates these layers of influence in a comprehensive framework.
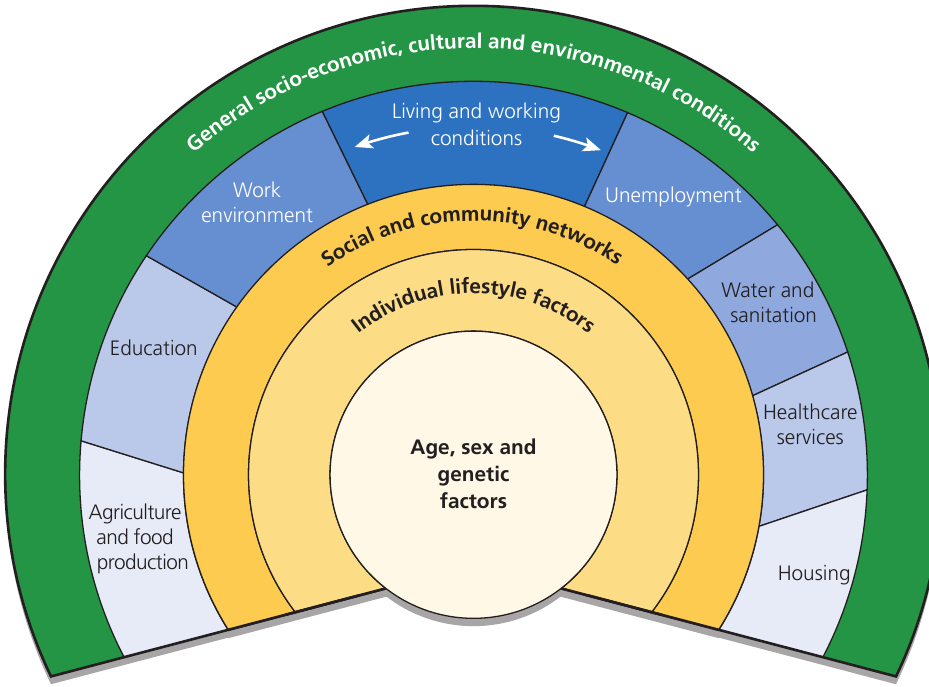
The model shows health determinants organised in concentric layers:
Individual level (centre):
- Age, sex and genetic factors form the core
- These are fixed characteristics that influence baseline health
Lifestyle level:
- Individual lifestyle choices and behaviours
- Personal decisions about diet, exercise, smoking and alcohol consumption
Social and community networks:
- Relationships with family, friends and community
- Social support systems and community engagement
- These connections significantly impact both physical and mental health
Living and working conditions: This layer includes multiple environmental factors:
- Work environment and employment status
- Education access and quality
- Housing conditions
- Healthcare services availability
- Water and sanitation infrastructure
- Agriculture and food production systems
Broader conditions (outer layer):
- General socio-economic, cultural and environmental conditions
- These overarching factors shape all other determinants
This model demonstrates that improving health requires action across all these levels. Individual behaviours matter, but they occur within contexts shaped by social, economic and environmental conditions largely outside personal control.
Global patterns of health, mortality and morbidity
Health is distributed unequally across the world. Significant disparities exist between countries at different stages of economic development, and these patterns reflect underlying inequalities in living conditions, healthcare access and environmental factors.
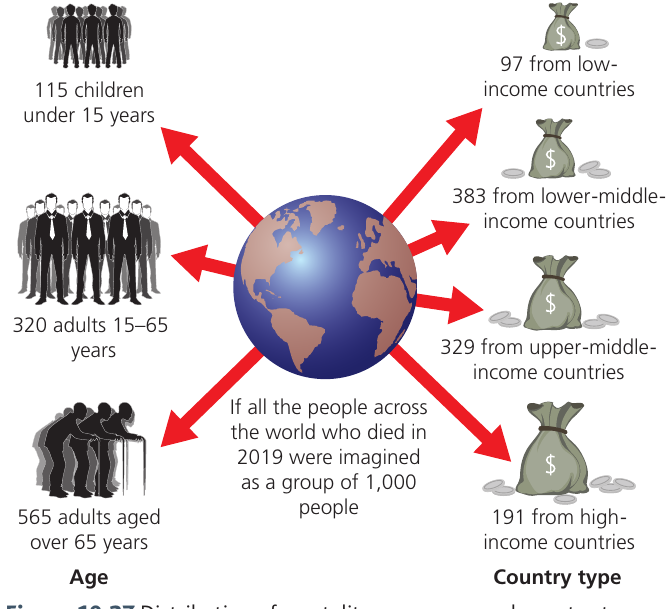
When examining global mortality in 2019, clear patterns emerge. If we imagine all people who died that year as a group of 1,000 individuals, the distribution reveals stark inequalities:
By country income level:
- 97 deaths occurred in low-income countries
- 383 deaths in lower-middle-income countries
- 329 deaths in upper-middle-income countries
- 191 deaths in high-income countries
This distribution shows that mortality rates are considerably higher in low- and middle-income countries. More than half (540 out of 1,000) of these deaths occurred in low- and middle-income countries combined, highlighting the disproportionate burden of disease in less developed regions.
By age group:
- 115 were children under 15 years
- 320 were adults aged 15-65 years
- 565 were adults over 65 years
The age distribution shows that the majority of deaths occur among older adults, reflecting the global trend towards populations living longer but eventually succumbing to age-related conditions.
Leading causes of death globally
The pattern of what kills people has changed significantly over recent decades. Comparing the top 10 causes of death between 2000 and 2016 reveals important shifts in global health challenges.
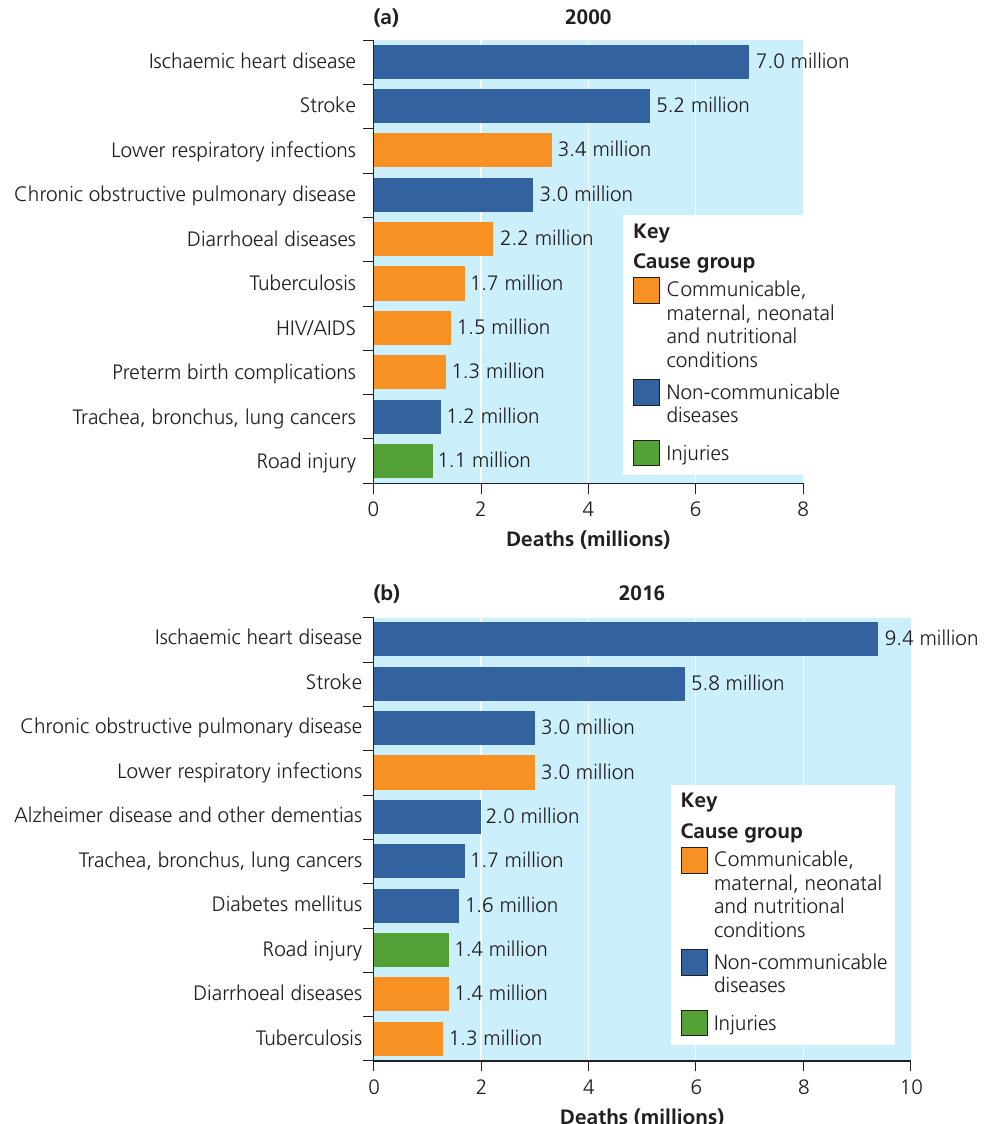
The rise of non-communicable diseases:
By 2018, NCDs accounted for 71% of all deaths globally, up from 60% in 2000. The four main NCDs driving this trend are:
- Cardiovascular diseases (heart disease and stroke)
- Cancers
- Diabetes
- Chronic respiratory diseases
In 2000, ischaemic heart disease was already the leading cause, causing 7.0 million deaths. By 2016, this had increased to 9.4 million deaths. Similarly, stroke deaths rose from 5.2 million to 5.8 million over the same period.
New conditions entered the top 10 by 2016, including Alzheimer's disease and other dementias (2.0 million deaths) and diabetes mellitus (1.6 million deaths), reflecting both ageing populations and lifestyle changes.
The decline of communicable diseases:
Deaths from infectious diseases have fallen substantially, reflecting improvements in sanitation, diet, medical treatments and medication. For example:
- Lower respiratory infections declined from 3.4 million deaths (2000) to 3.0 million (2016)
- Diarrhoeal diseases fell from 2.2 million to 1.4 million
- HIV/AIDS dropped from 1.5 million to outside the top 10 by 2016 (due to antiretroviral treatments)
- Tuberculosis decreased from 1.7 million to 1.3 million
Historically, deaths from infectious diseases were strongly associated with older age groups and occurred predominantly in high-income countries. However, WHO evidence from 2016 shows that low- and middle-income countries were disproportionately affected, with 32 million deaths (78% of all NCD deaths).
Notably, among the 41 million deaths from NCDs in 2016, 15 million people (36.5%) died between ages 30 and 69, indicating that NCDs are not solely diseases of old age.
The COVID-19 impact:
There was likely to be a significant spike in communicable disease deaths during 2020-21 due to the Coronavirus pandemic. The highly infectious COVID-19 virus caused over 1.7 million deaths by the end of 2020 alone. This lifted communicable diseases back into the top 10 causes of death for that year. Further waves of infection continued into 2021, affecting both high-income countries and developing nations. By early 2023, the global death toll exceeded 2.2 million, demonstrating that infectious diseases remain a significant threat even in the modern era.
Economic and social development
As societies and nations progress economically and socially, the conditions in which people live generally improve. This development process has profound effects on population health and healthcare provision.
Economic developments that improve health:
Economic progress creates multiple pathways to better health outcomes:
- Technology advances improve food productivity and supply. The Green Revolution, for example, dramatically increased agricultural yields, reducing malnutrition and famine-related deaths
- Enhanced transport infrastructure enables better distribution of food supplies and medical resources to remote or underserved areas
- Investment in drainage and sewage systems, particularly in urban areas, reduces the spread of water-borne diseases
- Trade in resources and manufactured goods allows countries to access a wider variety of foods and medicines, reducing nutritional deficiencies and improving treatment options
Social developments that improve health:
Social progress complements economic development:
- Improved awareness of hygiene practices helps prevent disease transmission. Public health campaigns educate communities about handwashing, food preparation and sanitation
- Better education about disease transmission enables people to protect themselves and their families from infectious conditions
- Advances in medical technology, such as antibiotics and vaccines, have dramatically reduced deaths from previously fatal infections
- Enhanced training for healthcare professionals (doctors, nurses and midwives) improves the quality of care
- Aid programmes from international organisations like the UN and NGOs help improve healthcare facilities, particularly in developing regions
The relationship with population growth:
Socio-economic development is typically accompanied by significant changes in population dynamics. Initially, as development begins, life expectancy increases and death rates decrease while fertility initially remains high. This creates rapid population growth.
Over time, as development continues, social norms change and families begin having fewer children. This occurs because:
- Healthcare improvements reduce infant mortality, so parents no longer need large families to ensure some children survive to adulthood
- Development brings improved access to contraception
- Economic changes mean children become an economic cost rather than providing labour
- Educational opportunities (especially for women) lead to delayed childbearing and smaller family sizes
This leads to subsequent declines in fertility rates, eventually stabilising population growth.
Epidemiological transition
The concept of epidemiological transition provides a framework for understanding how disease patterns change as countries develop. This theory was first proposed by Abdel Omran in 1971.
The core concept:
Omran suggested that the process of socio-economic development drives a fundamental transition in what causes death in populations. Countries move from a pattern where infectious diseases are the primary killers towards one where chronic, degenerative and lifestyle-based diseases dominate.
This transition occurs as a country undergoes modernisation from developing to developed nation status. It is a component of demographic transition and is driven by advances in medical technology, disease prevention and treatment for sickness.
The original three stages:
Omran identified three distinct phases in this transition:
Stage 1: The age of infection and famine
- Mortality rates are high and fluctuate considerably
- Population growth cannot be sustained due to high death rates
- The cyclical pattern of low growth is associated with wars, famine and epidemic outbreaks
- These periods of crisis are interspersed with brief periods of relative 'prosperity' when conditions temporarily improve
Stage 2: The age of receding pandemics
- Mortality rates begin to decline significantly
- Disease epidemics occur less frequently as public health measures improve
- Population growth becomes sustained and begins to rise exponentially
- This stage reflects improvements in sanitation, nutrition and basic healthcare
Stage 3: The age of degenerative and man-made diseases
- Mortality continues declining and eventually stabilises at a relatively low level
- Infectious agents are no longer the major contributors to morbidity and mortality
- Instead, chronic conditions linked to ageing and lifestyle become dominant causes of death
- These include heart disease, cancer, diabetes and respiratory conditions caused by factors like smoking and pollution
- Fertility becomes a more important factor driving population growth than mortality
The fourth stage:
During the 1980s, other public health researchers revisited and modified Omran's theory. Olshansky and Ault added a fourth stage:
Stage 4: The age of delayed degenerative diseases
- Death rates continue declining but become concentrated at advanced ages
- People live longer before succumbing to degenerative diseases
- Medical advances postpone death from chronic conditions
- Population ageing accelerates as more people survive into their 80s and beyond
Links to demographic transition:
The four recognised stages of epidemiological transition closely mirror the stages of the demographic transition model. Epidemiological transition is clearly one of the key factors explaining natural population change over time. As mortality patterns shift, they interact with changing fertility patterns to reshape population structures.
A fifth stage?
Since the 1980s establishment of the fourth stage, some researchers have suggested the world's population may be entering a fifth stage of epidemiological transition. This potential stage would reflect new patterns of disease emergence, including:
- Re-emergence of some infectious diseases due to antibiotic resistance
- New infectious diseases (emerging diseases like COVID-19)
- Mental health conditions becoming more prominent
- Lifestyle diseases continuing to rise, particularly obesity-related conditions
However, this fifth stage remains debated and is not yet universally recognised in the academic literature.
Key Points to Remember:
-
Health is multidimensional - it involves physical, mental and social wellbeing, not just the absence of disease. Multiple factors at individual, social and environmental levels determine health outcomes.
-
Global health is unequal - low- and middle-income countries experience disproportionately higher mortality rates. More than half of global deaths in 2019 occurred in these countries, reflecting underlying inequalities in healthcare access and living conditions.
-
Disease patterns have shifted - non-communicable diseases (especially heart disease, stroke, cancer and diabetes) now cause 71% of deaths globally, while deaths from communicable diseases have declined due to medical advances and improved sanitation.
-
Development improves health - economic and social development create better living conditions, improved nutrition, enhanced healthcare and reduced infectious disease transmission, though this is typically accompanied by significant population growth changes.
-
Epidemiological transition explains change - as countries develop, they move through predictable stages from infectious disease dominance to chronic disease dominance, mirroring the demographic transition and driven by improvements in medicine, technology and living standards.