Access and Equity and the Role of Australia’s Health System (VCE SSCE Health and Human Development): Revision Notes
Access and Equity and the Role of Australia’s Health System
Understanding how Australia's health system promotes health requires examining two key concepts: access and equity. While these terms are related, they address different aspects of healthcare delivery and fairness.
Access to healthcare
What is access?
A health system with good access ensures that all people can receive timely, quality health services based on their needs rather than their ability to pay. This means healthcare should be available to everyone, regardless of their income level or where they live in Australia—whether in major cities or remote areas.
Access is a fundamental principle because without it, people cannot benefit from healthcare services, no matter how high quality those services might be.
How Australia's health system promotes access
Australia's major healthcare programs work together to improve access for different population groups:
Medicare helps people from all socioeconomic backgrounds access essential services. It covers doctors' consultations and treatment in public hospitals. Additionally, Medicare now funds telephone and video consultations, which particularly benefit people living outside major cities who may struggle to see healthcare providers in person.
The Pharmaceutical Benefits Scheme (PBS) ensures all Australian citizens and permanent residents can access subsidised medicines. The PBS includes a concessional co-payment amount, making essential medicines more affordable for people on lower incomes.
The National Disability Insurance Scheme (NDIS) improves access to health services for people with significant, lifelong disabilities. Importantly, the NDIS has been rolled out across every region of Australia, helping people with disabilities access services regardless of location.
Private health insurance rebates from the federal government help lower-income Australians afford private health insurance, which can then provide access to health services that might otherwise be too expensive.
Barriers to access
Despite these programs, significant barriers to accessing healthcare remain.
Cost Remains a Major Barrier
According to the Australian Institute of Health and Welfare, almost one in five people (19 per cent) delayed or avoided visiting the dentist due to cost. When people delay medical treatment because they cannot afford it, their conditions can worsen, leading to more serious health problems down the track.
Many people struggle with the costs of:
- Patient co-payments for medical consultations
- Prescription medications
- Allied health services such as physiotherapy
- Ambulance transport and treatment
- Dental care
Geographic disparities in access
While the number of medical practitioners per 100,000 population has increased overall in Australia, access varies significantly by location. Although general practitioner numbers are relatively similar across regions, people in major cities have much greater access to specialists and other health professionals.
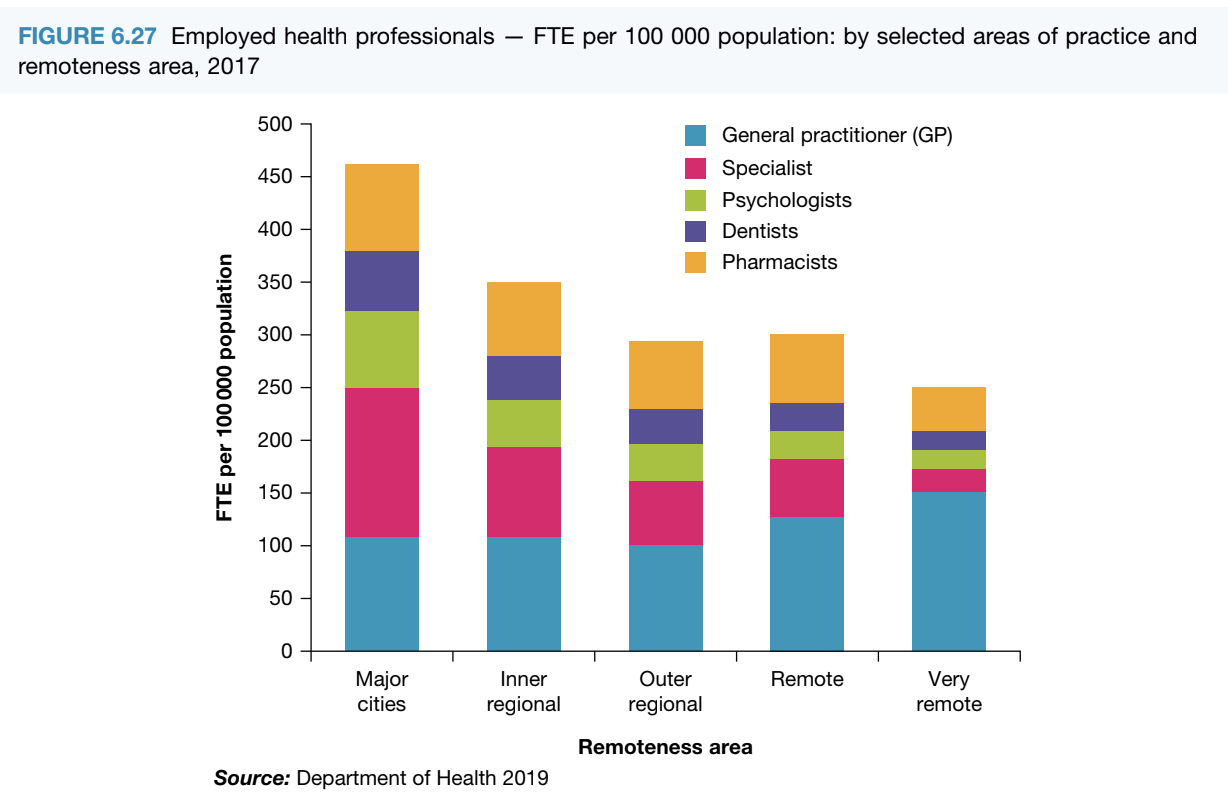
This chart reveals a clear pattern: as you move from major cities to very remote areas, the total number of healthcare professionals decreases dramatically. Specialists, in particular, are concentrated in major cities, leaving people in regional and remote areas with limited access to specialised care.
Improving access through targeted programs
Several programs work to address these geographic and financial barriers:
Royal Flying Doctor Service
This non-government organisation provides healthcare to thousands of Australians living outside major cities. The service receives funding from federal and state/territory governments to maintain its fleet of aircraft and road vehicles, enabling it to reach and treat people in remote locations.
Workforce Incentive Program
This federal government strategy offers financial incentives to doctors who work in rural and remote areas. By encouraging medical professionals to practice in underserviced regions, it helps improve healthcare access for people living outside Australia's major cities.
Culturally appropriate healthcare
Access means more than just physical availability—it also includes cultural appropriateness. This is particularly important for Aboriginal and Torres Strait Islander peoples, who may face additional barriers in mainstream healthcare settings.

The Indigenous Health Incentive provides financial support to medical practices that deliver culturally appropriate healthcare to Aboriginal and Torres Strait Islander peoples. This might include employing Indigenous health workers or adapting service delivery to respect cultural practices and preferences.
The Close the Gap initiative has invested in strategies outlined in the National Aboriginal and Torres Strait Islander Health Plan 2013–2023, including:
- Additional training for Aboriginal and Torres Strait Islander health workers
- Collaboration with Aboriginal and Torres Strait Islander groups and leaders to plan service delivery
- Culturally appropriate health promotion and education
While these initiatives have improved access to culturally appropriate healthcare, many Aboriginal and Torres Strait Islander people still lack adequate access. This ongoing gap contributes to differences in health status between Aboriginal and Torres Strait Islander peoples and other Australians.
Equity in healthcare
Understanding equity versus equality
It's important to understand that access and equity are different concepts. While access focuses on whether people can reach healthcare services, equity considers whether the system fairly meets different people's needs.
Equity vs Equality: A Critical Distinction
Equality means treating everyone the same way—giving everyone equal access to services. However, this doesn't necessarily lead to fair outcomes because people have different healthcare needs.
Equity means recognising these differences and responding appropriately. An equitable health system takes into account that some people face greater disadvantages or have more complex needs, and it provides additional support where needed.
For example, someone with a chronic illness may need more frequent medical care than a healthy person. An equitable system recognises this difference and provides additional support through mechanisms like the Medicare Safety Net, rather than treating both people identically.
Factors contributing to health disadvantage
Several factors can disadvantage people in using the health system:
- Chronic illness requiring ongoing care
- Poverty and financial hardship
- Discrimination based on background or characteristics
- Limited access to goods and services
- Language barriers
- Mental health conditions
- Disability
An equitable health system must recognise and respond to these special needs to ensure fairness for all people.
How Australia's health system promotes equity
The major healthcare programs include specific equity measures:
Medicare equity measures
Medicare Safety Net: People who need frequent Medicare-covered services (like doctor's visits and medical tests) receive additional financial support once they reach a certain threshold of out-of-pocket costs. This prevents people with greater healthcare needs from facing overwhelming expenses.
Mental Health Treatment Plans: People with mental health disorders can access 10 individual and 10 group therapy sessions per calendar year with Medicare covering the cost. This recognises that mental health is as important as physical health and shouldn't be a financial burden.
PBS equity measures
PBS Safety Net: This provides further protection for individuals and families from large overall medication expenses. Once you've spent a certain amount on PBS medicines in a calendar year, you pay less for each additional medicine.
Concessional co-payment: The reduced co-payment amount for PBS medicines provides greater assistance to people who are unemployed or on low incomes, recognising their limited financial resources.
Closing the Gap PBS co-payments: Many Aboriginal and Torres Strait Islander peoples qualify for reduced PBS co-payment amounts under the Closing the Gap initiative, acknowledging historical disadvantage and ongoing health inequities.
NDIS equity measures
The individualised plan at the heart of the NDIS ensures that people with more significant needs receive more assistance. Importantly, people who require NDIS support don't pay more towards funding it than those who don't need it—funding comes from general taxation, distributing the cost across all taxpayers regardless of their own disability status.
Private health insurance equity measures
The private health insurance rebate is income-tested, meaning people on lower incomes receive more financial assistance. Additionally, people aged 65 and over (who often have lower incomes and higher healthcare needs) receive a greater rebate from the government. Furthermore, people who use their private health insurance frequently don't have to pay higher premiums than those who rarely use it—the cost is spread across all policy holders.
Additional equity interventions
Beyond the major programs, other interventions promote equity:
Public dental health services
The Victorian Government funds the Royal Dental Hospital of Melbourne and over 80 dental clinics across metropolitan and regional Victoria. These provide dental treatment that is generally free for vulnerable groups, including:
- Young people aged 13–17 who hold healthcare or pensioner concession cards, or are dependents of cardholders
- Youth justice clients in custodial care, up to 18 years of age
- Refugees and asylum seekers
- Aboriginal and Torres Strait Islander peoples
This addresses the equity issue that dental care, while essential for health, often requires substantial out-of-pocket payment that disadvantages vulnerable populations.
Continuity of care
Continuity between healthcare providers aims to increase communication and care planning between different health professionals. This makes healthcare more manageable for patients with multiple healthcare needs.
Practical Example: Cancer Patient Care Coordination
A cancer patient might be under the care of a general practitioner and several specialists (oncologist, surgeon, radiologist). Good communication between these professionals ensures coordinated care, preventing the patient from having to repeatedly explain their situation and reducing the risk of conflicting treatments.
This promotes equity for people with serious illness by making the system easier to navigate.
Impact on health outcomes
These access and equity measures contribute to improved health outcomes across Australia by:
- Reducing financial barriers to essential healthcare
- Ensuring geographic location doesn't determine health outcomes
- Providing additional support for those with greater needs
- Recognising and addressing cultural differences in healthcare delivery
- Protecting vulnerable populations from healthcare costs
However, ongoing challenges remain. Continued efforts are needed to address persistent inequities, particularly for Aboriginal and Torres Strait Islander peoples, people in remote areas, and those experiencing financial hardship.
Key Points to Remember
- Access means people can reach healthcare services when needed, regardless of income or location, while equity means the system fairly responds to different people's needs
- Medicare, PBS, NDIS and private health insurance all include specific measures to promote both access and equity
- Geographic location significantly affects access to healthcare, particularly specialist services, with major cities having much better access than remote areas
- Safety nets in Medicare and PBS provide additional support when people have high healthcare costs
- Culturally appropriate healthcare is essential for equity, particularly for Aboriginal and Torres Strait Islander peoples
- Cost remains a significant barrier to accessing some healthcare services, particularly dental care and allied health services