What Areas of Youth Health and Wellbeing Need Action? (VCE SSCE Health and Human Development): Revision Notes
What Areas of Youth Health and Wellbeing Need Action?
Introduction
The transition from youth to adulthood is a critical period for health and wellbeing. The World Health Organization recognises that young people during this stage take increasing responsibility for their own health. As they move towards adulthood, young people interact with various environments that provide essential elements for a healthy life, including positive family relationships, quality education, strong social connections, respectful relationships, meaningful work, enjoyable leisure activities and healthy lifestyle choices.

Understanding the factors that influence youth health during this transitional period is essential for developing effective interventions and support systems that will benefit young people throughout their lives.
Why invest in youth health and wellbeing?
Investing in youth health and wellbeing provides significant benefits across multiple dimensions:
Immediate benefits
- Promotion of positive behaviours such as good sleep habits and constructive risk-taking (like sport or drama)
- Early detection and treatment of problems such as substance use disorders or mental health issues
- Prevention of immediate health concerns
Long-term benefits
- Establishing healthy behaviours during youth (such as nutritious eating, physical activity and safe sexual practices) helps create patterns that continue into adulthood
- Reducing harmful exposures and behaviours (such as obesity, alcohol and tobacco use) decreases morbidity, disability and premature death in later life
- Maintaining successful health interventions from childhood
- Protecting the health and wellbeing of future offspring through promotion of emotional wellbeing and healthy practices
Health behaviours established during youth create patterns that persist into adulthood. Investing in youth health not only benefits current wellbeing but also reduces the burden of disease across the entire lifespan.
Current health status
Over 90 per cent of Australian youth rate their health as either good, very good or excellent. However, data reveals areas requiring improvement. In 2018, whilst 67.6 per cent of young Australians aged 15 to 24 rated their health as excellent or very good, and 24.3% rated it as good, 7.9% rated their health as fair or poor. These lower ratings often involve risk factors that commonly emerge or increase during youth, which can affect both current and future health and wellbeing.
Understanding health inequalities among young people
Health inequalities are differences in health status or in the distribution of health risk and protective factors. These inequalities exist among young people in Australia as a cohort and between young people and other age groups. Health inequalities may result from sociocultural factors such as income, education, community expectations or gender that are avoidable or unfair. These are called social inequalities.
Disadvantaged communities
The Dropping Off The Edge research programme identifies the most disadvantaged suburbs and local government areas across Australia. Young people in disadvantaged communities experience:
- Higher rates of social exclusion
- Fewer opportunities for improving their circumstances
- Higher rates of low birth weight, childhood injuries and domestic violence
- Lower rates of immunisation
- Limited access to sports clubs, libraries and recreational facilities
- Schools less likely to offer extracurricular activities
- Difficulty affording registration fees, uniforms, equipment and transport
Social exclusion occurs when an individual is unable to participate fully in social and economic life, such as not having a job, not receiving adequate income, not getting good education or not being connected to family, friends and the community.
Opportunity structures
Affluent suburbs tend to have good opportunity structures - a combination of physical facilities and social networks that provide access to education, jobs and other opportunities. Low-income suburbs often lack these opportunity structures, creating significant disadvantages for young people.
Risk and protective factors
Youth health inequalities arise from variations in exposure to risk and protective factors:
- Risk factors are elements that increase the likelihood of developing disease or injury
- Protective factors enhance the likelihood of positive health and wellbeing outcomes and lessen the likelihood of negative outcomes from exposure to risk
Health inequalities in youth can result from risk-taking behaviour and inexperience. These can be addressed by:
- Empowering youth to change behaviour
- Government action
- Early intervention to promote protective factors
- Health promotion programmes
- Strengthening protective factors
Taking health action
Health action involves making health behaviour changes by replacing health-compromising behaviours (such as sedentary behaviour) with health-enhancing behaviours (such as physical exercise). This is more likely to succeed when we plan when, where and how to undertake the desired change.
Action plan framework
Action plans spell out small and realistic steps for addressing a health goal. They can be used for various goals including stopping smoking, reducing stress, improving sleep habits and changing diet or physical activity routines. Research shows that most people who make an action plan experience greater success at making associated behaviour changes.
Action Plan Framework
An effective action plan includes:
- Health goal - what you want to achieve
- Actions - what you need to do to achieve your goal
- Success indicators - milestones that show you're on the right track
- Start/Finish - when you will start and finish working on your goal
For example, if your goal is to improve sleep habits:
- Goal: Get 8 hours of sleep per night
- Actions: Set bedtime routine, avoid screens 1 hour before bed, maintain consistent sleep schedule
- Success indicators: Feeling more alert during the day, falling asleep within 20 minutes
- Timeline: Start next Monday, review progress after 2 weeks
Youth concerns and priorities
The Mission Australia Youth Survey provides annual feedback from young Australians aged 15 to 19 about the issues that concern them. This information informs government action, policy and the work of community organisations. The survey data helps identify which aspects of youth health and wellbeing require action.
Areas of youth health and wellbeing requiring action
Based on health data and youth concerns, the following areas have been identified as requiring health action:
Key Areas Requiring Action:
- Injury
- Alcohol use
- Illicit use of drugs
- Smoking
- Weight issues
- Sexual health
- Stress and mental health
- Discrimination
These areas are not meant to provide exhaustive detail, but rather sufficient information to understand the key issues affecting young Australians.
Injury
Injury is an umbrella term referring to a range of causes of mortality and morbidity, including traffic accidents, suicide and poisoning, falls, violence and drowning. Although death rates from injury have decreased significantly over the past 20 years, injury (which includes suicide) remains the leading cause of death for youth in Australia.

Impact of injury
All injuries are considered preventable, which can add to the impact they have on individuals. Serious outcomes from injury include:
Life-threatening outcomes (more common in road crashes):
- Spinal cord injury
- Traumatic brain injury
- Death
Non-life-threatening outcomes (more common in sport):
- Soft tissue sprains and strains
- Bone fractures
- Cuts
- Eye wounds
- Dislocations
Sporting injuries
Research by La Trobe University found that among patients who had undergone two knee reconstructions before age 25, the majority (91 per cent) played AFL, basketball, soccer or netball before their injury. More than one quarter (27%) had suffered three anterior cruciate ligament (ACL) injuries. Multiple ACL injuries affect the knee's main stabilising joint, putting young people at significant risk of developing knee osteoarthritis, which can have lifelong effects on their ability to remain active.
The incidence of ACL reconstructions in Australia is the highest in the world and is increasing. Those at greatest risk are men aged 20-24 years and women aged 15-19 years, with incidence increasing most rapidly among 5-14-year-old children.
Statistics and inequalities
Young people are over-represented in injury statistics compared with any other age group. Key statistics include:
Deaths
- Leading causes of death for 15-24 year olds: suicide (38.8%), land transport accidents (23.2%), accidental poisoning (5.9%), assault (2.4%)
- Land transport accidents are the main reason for hospitalisation of youth
Gender differences
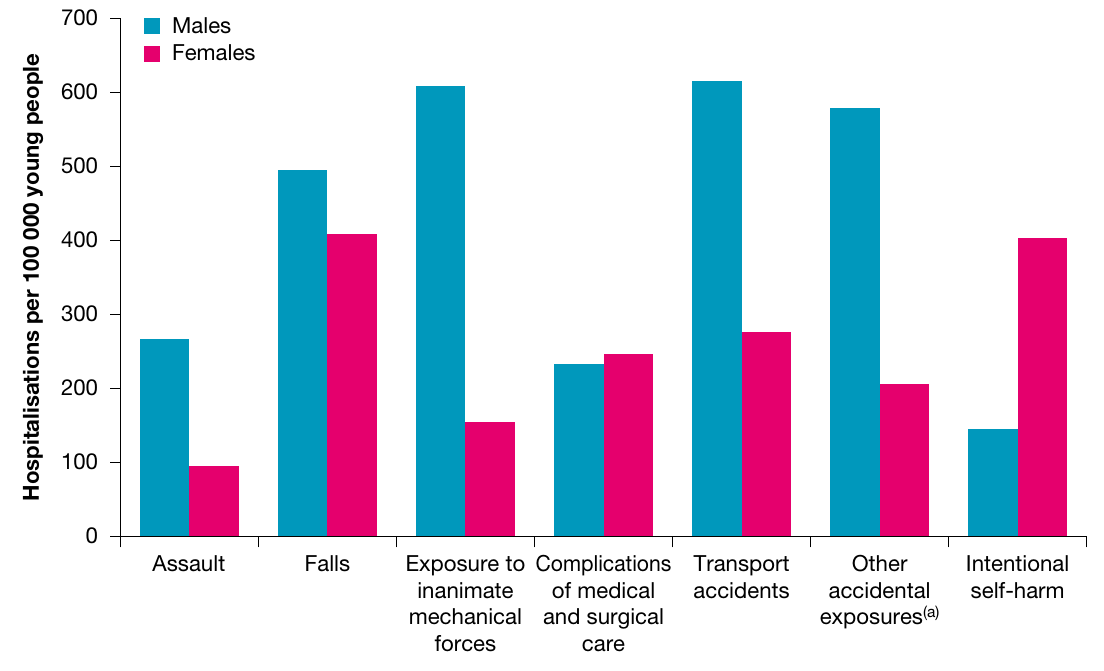
- The highest age-specific rate for road crash hospitalisation was for males aged 15-24 (321 cases per 100,000 population)
- Males are 1.9 times more likely to be hospitalised for injury or poisoning than females
- Females aged 15-24 are 2.8 times more likely to be hospitalised for self-harm than males aged 15-24
- Males are 2.2 times more likely to be hospitalised for transport accidents than females
Specific injuries
- 15-24 year olds have the highest age-specific rate of spinal cord injury (ratio of male to female injury is 9 to 1)
- Over the past 15 years, ACL sporting injuries and reconstructions in Australians under 25 have risen more than 70%, with greatest increase among children under 14
- 15-19 year old males are most at risk of traumatic brain injury (399 per 100,000 population compared to 189 per 100,000 for the general population)
Self-harm
- 24.4% of young women and 18.1% of young men aged 20-24 have self-injured in their lifetime
Workplace injuries
- Every four minutes and 24 seconds, on average, a young person is injured in an Australian workplace
Geographic and cultural differences
- Rural youth are more likely to engage in dangerous behaviours resulting in accidental injury than urban youth
- Indigenous children and young people are over one and a half times more likely to require hospitalisation for injuries
- Indigenous youth are six times more likely to die from assault and four times more likely to die from suicide than non-Indigenous youth
Contributing factors
The youth stage has specific relationships with both the type and rate of injuries experienced:
Developmental factors
- Areas of the brain controlling decision making and self-control are still developing
- Reward-processing and pleasure-seeking areas of the brain are also developing
- This can lead to more risk-taking behaviour
- Young people may use emotions to process information rather than thinking through consequences
The prefrontal cortex, which controls executive functions like planning and impulse control, doesn't fully mature until around age 25. This biological reality helps explain why young people are more prone to risk-taking behaviour.
Increased independence
- Greater mobility with less adult supervision
- New situations requiring development of new skills (employment, driving)
- Inexperience can have serious implications for injury
- Peer acceptance may motivate risk-taking over longer-term health concerns
Risk-taking behaviours
- Alcohol or drug consumption particularly significant
- Strong relationship with injury and death
- Young people may feel they will live forever
- Belief that "it couldn't happen to them"
- Limited attention spans and different concept of time
- Understatement of risks and overstatement of gains
Transport-related accidents
The over-representation of young people in transport-related accidents links to:
- Speeding
- Driving when fatigued
- Driving under the influence of alcohol or other drugs
- Inexperienced drivers with lowered hazard perception
- Still-developing brain
- Driving at night
- Presence of other young passengers
Young drivers place themselves at greater risk by:
- What they drive - young drivers sharing mum and dad's car are less risky on the road
- When they drive - driving in risky circumstances (at night or when tired)
- How they drive - speeding, not wearing seatbelts, making driving errors
- Why they drive - changing driving behaviour based on emotional state
Sporting injuries
Increased incidence thought to result from:
- Earlier specialisation at younger ages
- Longer sporting seasons
- More intense training
- Higher levels of competition
- Lack of free play
Workplace injuries
Young workers face increased risks when:
- Required to perform duties without adequate training
- Little supervision in the workplace
- Making decisions for which they are ill-equipped
- Using dangerous equipment
- In casual and temporary jobs without sufficient time for proper training
- Concerned about losing their job if they complain
Rural areas
Higher likelihood of injury may relate to:
- Poor quality roads
- Longer distances to travel
- Less safe vehicles
- Lower health literacy about accident prevention (the degree to which individuals have the capacity to obtain, process and understand basic health information needed to make appropriate decisions)
- Lower compliance with safety regulations, speed limits, use of seat belts and vehicle roadworthiness
Alcohol use
Youth is a stage when many people experiment with alcohol. Youth under age 18 are recommended not to consume any alcohol as their bodies and brains are experiencing rapid development, particularly:
- The hippocampus (involved in memory and learning)
- The prefrontal cortex (controls planning, judgement, decision making and impulse control)
The brain continues to develop through young adulthood up until around age 25. Alcohol consumption during this critical developmental period can have lasting effects on brain structure and function.

Alcohol guidelines
For youth aged 18 and over, to reduce the risk associated with alcohol consumption, the Department of Health and Ageing recommends not consuming more than:
- Two standard drinks on any day (to reduce lifetime risk)
- Four standard drinks on any day (to reduce short-term risks)
Effects of alcohol
Alcohol can:
- Reduce alertness and concentration
- Reduce coordination skills and problem-solving ability
- Promote risk-taking behaviours, including self-harm
- Increase aggression
- Reduce ability to accurately assess risks to safety
- Lower levels of self-control
- Reduce ability to identify hazards and dangers
Young people under the influence of alcohol are less able to accurately assess risks to their own safety and that of others. This can lead to unsafe sex, physically dangerous behaviour, and driving or getting in a car with someone who is drunk.
Binge drinking
Binge drinking (consuming seven or more standard drinks for males or five or more standard drinks for females in one sitting) during youth is associated with:
- Higher rates of injury, death and violence-related trauma
- Cuts and concussions
- Affected brain development (memory, learning ability, verbal skills)
- Increased risk of alcohol-related problems later in life, including alcohol dependence
- Mental health problems including depression, self-harm and suicide
Statistics and trends
Whilst there are worrying levels of alcohol use among some young people, there are encouraging statistics showing that young people are starting drinking later and some don't drink at all.
Positive trends
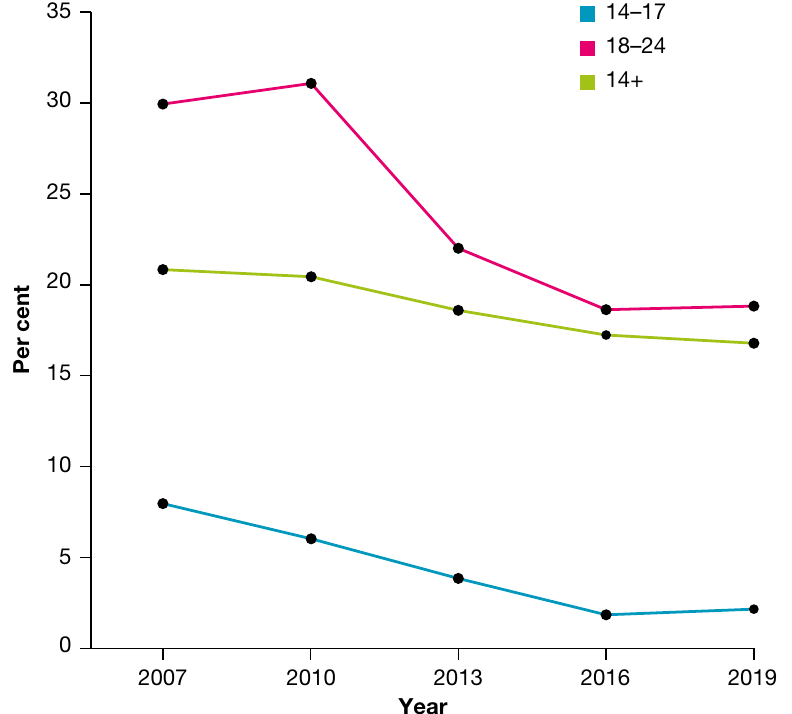
- Average age at which 15-24 year olds first consumed alcohol has steadily risen from 14.7 years in 2001 to 16.2 in 2019
- Proportion of 14-17 year olds who abstained increased from 39% (2007) to 73% (2019)
- Proportion of 18-24 year olds who abstained rose from 13.1% (2007) to 21% (2019)
Gender differences
- Proportion of males exceeding risk guidelines increased from 23% (2016) to 27% (2019)
- Proportion of females exceeding risk guidelines decreased from 12.9% (2016) to 9.7% (2019)
- People aged 18-24 (14.6%) were more likely to consume 11 or more standard drinks at least monthly than other age groups
Regional and cultural differences
- Young people (including underage drinkers) in regional Victoria routinely drink at levels that put them at high risk compared with metropolitan areas
- 28.1% of Aboriginal and Torres Strait Islander young people identified alcohol and drugs as an important issue, compared with 20.3% of non-Indigenous young people
Research findings:
- Young people who drink weekly before age 17 are two to three times more likely to binge drink, drink drive and be dependent on alcohol in adulthood
- Alcohol contributes to the three major causes of teen death: injury, homicide and suicide
Contributing factors
A young person's decision to drink alcohol can be influenced by:
Family factors
- Early introduction and access to alcohol
- Parental attitudes to alcohol
- Many parents believe serving alcohol at home teaches responsible drinking, but research indicates children whose families refused to serve them alcohol at home were less likely to drink in other situations
- Young people exposed to close family members drinking or getting drunk are more likely to use alcohol
- Less supervision or excessive control
- Family conflict
Social and cultural factors
- Friends who drink heavily
- Australia's drinking culture (alcohol present in many social situations, such as sporting events)
- Belief that all young people drink (despite research showing they don't)
- Belief that drinking helps them fit in or provides confidence for social situations
- Seeing celebrities or role models drinking creates assumption it's socially desirable
- Access to cheap alcohol
- Alcohol marketing and advertising
Individual factors
- Poor educational achievement
- Income
- Long periods of free time
Current research
Recent research supports that public health messages should focus on drinking frequency rather than just amount consumed. Messages should recommend less frequent drinking rather than only focusing on quantity.
Rural context
Some young people in rural Australia associate drinking with values such as 'self-reliance', 'hardiness' and 'mateship'. Rural young people experience disproportionately high levels of alcohol misuse, possibly due to:
- Lack of venues for recreation (local sports clubs and their bars are among few leisure venues)
- Attitudes about help-seeking
- Economic and employment disadvantage
- Less access to healthcare professionals and alcohol treatment services
- High levels of boredom in leisure hours
- Lack of knowledge of alcohol guidelines and alcohol-related harm
- Easier access to alcohol
- Low level of community awareness of alcohol as a problem
Illicit use of drugs
Many people experiment with drugs and other substances during youth. Illicit use of drugs involves use of an illegal drug (prohibited from manufacture, sale or possession) or misuse of a legally available drug.
Effects and consequences
Illicit drug use can lead to a range of short and long-term effects on health and wellbeing:
Health effects
- Internal organ damage (including brain damage)
- Depression
- Mental disorders
- Increased rate of substance abuse issues later in life
Social consequences
- Social isolation
- Poor academic performance
- Unemployment
- Increased criminal behaviour
- Family breakdown
Common substances used during youth
- Marijuana (cannabis)
- Amphetamines (including ecstasy and crystal meth)
- Cocaine
- Heroin
Young people may also experience health concerns caused by others' harmful drug-taking behaviour, including drug-related violence at home or in public places, parental and peer substance use, and others' risk-taking behaviours such as driving under the influence of drugs.
Statistics and trends
There has been an overall reduction in the proportion of people in younger age groups reporting recent use of illicit drugs:
- Average age at which people first tried any illicit drug was 19.9 years in 2019 (oldest in 18 years)
- 9.7% of young people aged 14-17 had used illicit drugs in previous 12 months in 2019 (significantly less than 10.9% in 2016)
- Cannabis was the most used illicit substance: 16% of students aged 12-17 had ever used cannabis, and 8% used it in the month before the survey
- 6.3% of 14-19 year olds misused pharmaceuticals in 2019
- 20.8% of young people nominated alcohol and drugs as a key issue facing Australia in 2019, which decreased to 10.5% in 2020
Contributing factors
The reasons for youth trying drugs are complex. Like most risk-taking behaviours, drug use arises from a combination of factors:
Social factors
- Peer group pressure
- Fear of not being accepted into a social circle that includes drug-using peers
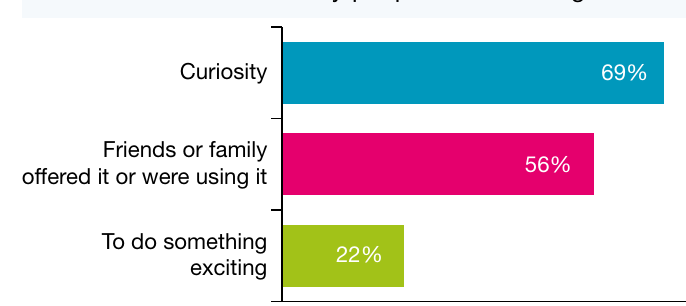
- Friends or family offering it or using it (56% of first-time users)
- Social exclusion
Individual factors
- Curiosity (69% of first-time users)
- Seeking new experiences and excitement (22% of first-time users)
- Drugs interact with brain chemistry to produce feelings of pleasure
- Lessening feelings of distress from depression, social anxiety and stress-related disorders
- Low mood
Young people may use drugs because they produce feelings of pleasure and lessen feelings of distress that may arise from depression, social anxiety and stress-related disorders. Understanding these underlying motivations is crucial for effective prevention and intervention strategies.
Smoking
Youth is a critical time in the development of tobacco addiction. Those who do not smoke during youth are less likely to smoke later in life.
Nicotine addiction
Nicotine is the addictive drug in tobacco smoke. Research shows:
- Symptoms of addiction (craving and withdrawal) can begin when youth smoke as few as two cigarettes a week
- Young people can develop nicotine addiction on average within two months of starting to smoke
- Some report symptoms of dependence even before they start smoking on a daily basis
E-cigarettes and vaping
E-cigarettes are battery-powered devices that heat a liquid to deliver vapour that can contain nicotine or flavours. People who use these are said to be 'vaping'. In Australia, commercial sale by retail outlets of nicotine e-cigarettes or liquid nicotine for vaping (e-liquid) is illegal.
E-cigarettes threaten to undermine public health measures to reduce smoking because:
- They could be doing it right under parents' noses (no odour or taste)
- They can be easily disguised (look like highlighters, USB drives, pens)
- Kids can consume them quickly (one vape could contain as much as two and a half packs of cigarettes)
- Social media marketing is particularly powerful among teens
- They are cheap and easily accessible (around $15)
- Most parents don't know they exist
- Vaping is an introduction to cigarettes, setting up youth to smoke later in life
- Unknown health repercussions from chemicals used
Health consequences
Smoking increases chances of:
- Premature death
- Cancer
- Cardiovascular disease
- Respiratory illness
Even though 2020 data shows smoking rates (11.6%) have halved since 1991 (25%), tobacco use is the single most preventable cause of ill-health and death in Australia, contributing an estimated 7.8% of the total burden of disease. This equates to more drug-related hospitalisations and deaths than alcohol and illicit use of drugs combined.
Statistics and trends
Rates of smoking among young people are extremely low:
Positive trends
- Average age at which 14-24 year olds smoked their first full cigarette increased from 15.4 years (2010) to 16.6 (2019)
- Adolescents aged 14-17 and young adults aged 18-24 were more likely to have never smoked than any other age group (97% and 80% respectively in 2019)
- This represents an increase from 2001 (82% and 58% respectively)
E-cigarette use
- E-cigarette use was higher among younger age groups
- 64% of smokers aged 18-24 tried an e-cigarette in their lifetime, compared with 26% of smokers aged 60-69
Indigenous youth
- Indigenous youth 15-17 years are more likely to be daily smokers
- In 2018-19, 11.7% of Aboriginal and Torres Strait Islander males and 7.8% of females were daily smokers
- Compared to 2.4% of non-Indigenous males and 1.1% non-Indigenous females
- Although smoking prevalence among Indigenous Australians has been declining in both non-remote and remote areas, most change has occurred in non-remote areas
Contributing factors
The decline in young people smoking may result from:
- Public awareness campaigns
- Tighter restrictions around smoking in public spaces
- Greater regulations around legal purchasing age
- Increased costs of cigarettes
Despite vast information about health consequences, some young people continue to smoke because:
- They don't perceive themselves as personally at risk
- They may underestimate the risk relative to other behaviours
- Number of close friends who smoke
- Whether parents smoke
- Exposure to tobacco advertising (though this is illegal in Australia, product placement still occurs)
Weight issues
To maintain a stable weight, young people need an energy (kilojoule) intake that equals their energy use. If they use more energy than they consume, they will lose weight. If they consume more kilojoules than needed for growth and activity, they will gain weight.
Being underweight
Being underweight can lead to:
- Weakened immune system
- Increased risk of infection and disease
- Inability to concentrate at school due to low energy levels
- Stress and problems with schoolwork affecting mental and emotional health and wellbeing
- Delayed puberty
- Required increases in bone and muscle mass may not be achieved
Obesity
Obesity in youth can have lifelong implications and contribute to many leading causes of death among adults.
Short-term effects
- Psychological distress
- Sleeping problems
- Low levels of energy
- Social problems (bullying, negative stereotypes, discrimination, social marginalisation)
- Reduced mental health and wellbeing (low self-esteem, low self-confidence, negative body image)
- Exclusion from competitive physical activities
Long-term risks
- Cardiovascular disease
- Type 2 diabetes
- Arthritis
- Some cancers

The increased prevalence of overweight and obesity among youth is due to combination of changes to food intake and development of sedentary lifestyles.
Statistics and trends
Overweight and obesity has become a major health and wellbeing concern for Australian youth, particularly for those who live outside major cities:
Current statistics
- Rate of overweight and obesity has stabilised but is still high
- In 2017-18, 1 in 4 (25%) Australian children and adolescents aged 2-17 were overweight or obese
- 1 in 12 (8.2%) were obese
Inequalities
- Aboriginal and Torres Strait Islander children and adolescents, those with disability, those in inner regional areas, and those in lowest socioeconomic areas are more likely to be overweight or obese
- In 2017-18, 2-17 year olds living in lowest socioeconomic areas were more than twice as likely to be obese as those in highest socioeconomic areas (11% compared with 4.4%)
- Although overweight and obesity rates for all Australian children and adolescents have plateaued since 2007-08, rates for Indigenous children and adolescents increased from 31% (2012-13) to 38% (2018-19)
- Biggest increase was for children aged 5-9 (from 27% to 36%)
Body image concerns
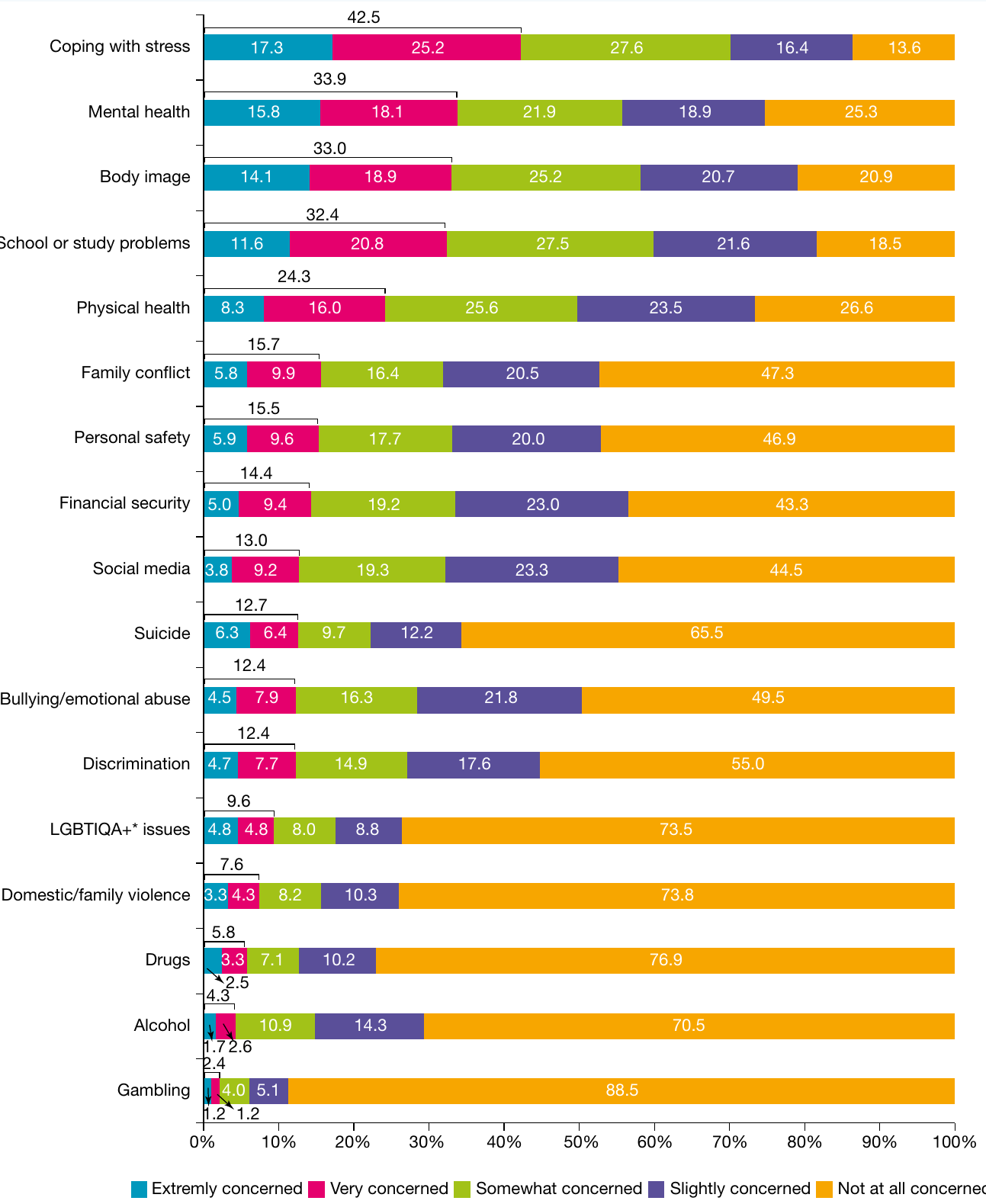
- Three in ten respondents to Mission Australia Youth Survey were either extremely or very concerned about body image (31.0%)
- Around twice the proportion of Aboriginal and Torres Strait Islander females were extremely or very concerned about body image (42.9% compared with 18.7% of males)
Contributing factors
An increase in obesity results from an imbalance between energy intake and expenditure.
Dietary factors
- Poor diet and snack choices
- Sugary beverages
- Increased portion sizes
- High intake of processed snack food
Physical activity factors
- Sedentary lifestyles
- Increased electronic and small screen recreation
- 58% of students have at least three televisions in their home
- 40% have video games in bedrooms
- More than three-quarters of teenagers spending more than two hours in front of computers, laptops, tablets, video games and televisions every school day
Environmental factors
- Safety concerns of parents reducing walking to school
- Poor urban planning
Whilst genetics can play a role in obesity development, it is not the cause of recent increases in early obesity. The rapid rise in obesity rates points to environmental and lifestyle factors as the primary drivers.
Sexual health
Sexual health is a state of physical, mental and social wellbeing linked to sexuality. It is not only about sexually transmitted infections but also about sexual relationships, safety and respect. Youth is often a time of sexual exploration, which can have both short and long-term effects on health and wellbeing.
Sexual health components
According to the World Health Organization, sexual health requires:
- A positive and respectful approach to sexuality and sexual relationships
- Possibility of safe sexual experiences, free of coercion, discrimination and violence
- Respect and protection of sexual rights of all young people
- Understanding how your body functions
- Being comfortable with your own body and sexuality
- Ability to form healthy relationships
- Being able to recognise and reduce risks, act responsibly, and set appropriate boundaries
- Communicating with people you have relationships with
- Knowing how to access and use healthcare services and information
Sexually transmitted infections (STIs)
STIs (sexually transmitted or transmissible infections) pass from one person to another through sexual contact, including oral, genital and anal sex.
Chlamydia
- By far the most common treatable sexually transmitted infection
- Notifications continue to increase each year
- Risk is highest in people aged 15 to 24
- 80% of cases occur in this age group
- Many STIs may not have obvious symptoms, so treatment is often not sought
Short and long-term effects
- Infections and chronic pain in cervix, pelvis and uterus (females)
- Effects on testes, urethra and prostate (males)
- Some STIs (herpes and HIV) are incurable and can affect health and wellbeing for life
Respectful relationships
Respectful relationships do not involve:
- Someone forcing or pressuring a young person to engage in sexual activity
- Posing for sexually explicit photos
- Cyberbullying or sexting (using technology or social media to harass, intimidate or threaten someone)
If youth participate in unsafe sex, they may expose themselves to range of STIs and unintended pregnancy.
Statistics and trends
Pregnancy
- 6,885 births to teenage mothers in Australia in 2018, down from 11,865 in 2010
Chlamydia
- In 2020, chlamydia notification rates were highest in age groups 20-24 (1,291 per 100,000), 15-19 (777.7 per 100,000) and 25-29 (768.3 per 100,000)
- Over past five years, there has been decline in annual chlamydia notification rate among 15-19 year olds
Geographic differences
- Higher rates of STIs recorded in remote areas, where 81% of reported cases are 15-24 year olds
Indigenous youth
- Aboriginal and Torres Strait Islander teenagers aged 15-19 years had fertility rate five times the teenage fertility rate for all women (48.1 and 9.5 births per 1,000 women respectively)
Sexting
- The sixth National Survey of Australian Secondary Students and Sexual Health found that 54.7% of surveyed students reported receiving a sexually explicit text message
- 32% reported sending a sexually explicit photo or video of themselves
Contributing factors
According to the AIHW, youth may be at increased risk of STIs due to:
Knowledge and skills
- Lack of knowledge
- Inconsistency with condom use
- Lack of communication and negotiation skills making using condoms difficult
- 75% of young Australians aged 15-29 who had sex in the last year did so without a condom at least once
Partner factors
- Many young people have not decided on long-term partner
- Potential for STIs to spread at high rates in this age group
Prevention
- Avoiding sexual contact is safest way to prevent contracting STI
- For those who are sexually active, using condom during sexual contact can reduce risk
Rural context
Rural areas face specific challenges:
- Reduced access to condoms (supermarkets not stocking them or keeping them under counter, limited availability of free condoms, reluctance to maintain condom vending machines due to vandalism)
- Physical isolation
- Lack of public transport
- Lack of specialised services
- Fears about confidentiality
- Sometimes conservative local attitudes
Positive factors
The internet can give youth access to reliable and confidential information in areas where questions may be too hard to ask. Use of social media is almost universal and plays large role in negotiation and development of sexual relationships, though this may involve sending explicit messages and images, most of which appear to occur within relationships.
Stress and mental health
Stress is a response to pressure or a threat. Under stress, a person may feel tense, nervous or on edge. The stress response is a physical one: a surge of adrenaline temporarily affects the nervous system.
Characteristics of stress
Stress is characterised by feelings of:
- Tension
- Frustration
- Worry
- Sadness
- Withdrawal (of short duration)
The body uses energy to cope during frequent bouts of stress.
Effects of stress
Physical health effects
Although the link is still unclear and research is ongoing, there is evidence to suggest that stress may contribute to:
- Cardiovascular disease
- High blood pressure
- Increased risk of infection
- Chronic fatigue
Mental health effects
Extended periods of stress can lead to more serious psychological disorders such as:
- Depression
- Anxiety
Depression involves extreme feelings of hopelessness, sadness, isolation, worry, withdrawal and worthlessness that last for a prolonged period and interfere with normal activities. Depression is both severe and long lasting.
Statistics and trends
The data show that anxiety was the most common mental disorder among young people, and stress caused by schoolwork is rated highly:
Mental health disorders
- Nearly one in three young Australians (32%) aged 12-25 reports high or very high levels of psychological distress - more than treble the rate in 2007 (9%)
- 14% of young people aged 12-17 had a mental disorder in the last 12 months
- Anxiety was most common (7%), followed by Attention Deficit Hyperactivity Disorder (6.3%) and major depressive disorders (5%)
- One in four young people are living with a mental disorder
- 9% of young people aged 16-24 experience high to very high levels of psychological distress
Stress concerns
- In Mission Australia 2020 survey, coping with stress was a major concern for around six in ten (55.5%) females (extremely concerned: 23.4%; very concerned: 32.1%)
- Compared with around one quarter (24.8%) of males (extremely concerned: 8.4%; very concerned: 16.4%)
- For Aboriginal and Torres Strait Islander respondents, coping with stress was the top issue of concern, with 36.6% indicating they were either extremely concerned (16%) or very concerned (20.6%)
Contributing factors
Growing up and finding balance between independence and reliance on others can create stress and lead to serious depression for young people who are ill-equipped to cope, communicate and solve problems.
Primary sources of stress
- Relationships with friends and family
- Schoolwork (homework and assessment)
- Expectations from others (teachers, sports coaches)
- Problems in lives of family and friends
Effects on health behaviours
Feeling pressured or stressed by schoolwork may influence health and wellbeing and health behaviours. Stressed students can:
- Engage in more health-compromising behaviours (smoking, drinking alcohol)
- Have more frequent health concerns (headache, abdominal pain)
- Experience psychological problems (feeling sad, tense, nervous)
Social media impact
Heavy use of social media can create stress:
- Average 14-24 year old Australian female spends almost 14 hours on social media every week (nearly two hours daily)
- Males aged 14-24 spend average of just under 9 hours weekly
- 56% of Australian youth are heavy social media users
- 25% report being connected to social media constantly
Fear of Missing Out (FOMO)
- 50% of teens experience FOMO
- Characterised as feeling anxious that something exciting or interesting is happening elsewhere
- Approximately 45% feel their peers are having more rewarding experiences than them
- Social media can make anxiety worse when young people see posts about wonderful times friends are having without them
- Stress arises when they go on holidays or miss social opportunities and don't know what friends are doing
Sleep disruption
Studies have found that access to and use of mobile devices at bedtime were associated with "poor sleep quantity" which can lead to mental and physical health and wellbeing problems:
- Obesity
- Poor academic achievement
- Daytime sleepiness
Positive aspects of social media
Despite negative impacts, social media can:
- Help psychologists monitor mental health and wellbeing of patients
- Help spread awareness about issues including mental disorders
- Connect people with one another
Discrimination

Discrimination occurs when a person or group of people is treated differently based on one of their characteristics such as their sex, culture or sexual orientation.
Types of discrimination
Ethnic and race-based discrimination
- Based on perceived 'racial' differences, culture, religion or language
Gender identity discrimination
- When a person is treated less favourably than another person in similar situation because of that person's gender-related identity, appearance, mannerisms or other gender-related characteristics
Around one in four young people aged 15 to 19 years report they have experienced unfair treatment or discrimination, with three main reasons reported as gender, race/cultural background and age.
Effects of discrimination
Discrimination can have potentially negative impacts:
Mental health effects
- Creating stress and fear
- Reduced capacity to form social connections important for good mental health and wellbeing
- Trust in others undermined
Physical health effects
- Effects of stress on immune, endocrine and cardiovascular systems
Behavioural effects
- Affected individuals may attempt to manage stress by engaging in behaviours damaging to health (smoking, alcohol or illicit drug use)
Social effects
- May result in violence associated with poor physical and mental health and wellbeing
- Social isolation and exclusion
Statistics and trends
Discrimination is a major issue for young people in Australia, particularly among Indigenous Australians:
Overall statistics
- Multicultural Youth Australian Census Status Report 2017/18 showed almost half of multicultural young people experienced some form of discrimination or unfair treatment in last 12 months (48.7%)
- Almost two thirds had witnessed someone else being unfairly treated or discriminated against (63.5%)
Indigenous youth
- Around one quarter of Aboriginal and Torres Strait Islander and non-Aboriginal or Torres Strait Islander young people identified equity and discrimination as important issue
- Aboriginal and Torres Strait Islander young people were almost twice as likely to report experiencing racial discrimination than non-Indigenous peers
Gender differences
- For non-Aboriginal or Torres Strait Islander young people, leading causes of discrimination were gender (39.1%) and race/cultural background (30.8%)
- Almost half of females who reported discrimination indicated this was on basis of gender
- Female students are more likely than males to have decreased health and wellbeing because of racism
LGBTIQ youth
- LGBTIQ (lesbian, gay, bisexual, transgender, intersex, questioning) young people report experiencing verbal homophobic abuse (61%), physical homophobic abuse (18%), and other types of homophobia (9%)
- Includes cyberbullying, graffiti, social exclusion and humiliation
Recent trends
- In Mission Australia 2020 survey, discrimination was listed as concern by 40.2% of non-Indigenous respondents (up from 24.8% in 2019)
- 37.9% of Indigenous respondents concerned (up from 24.3% in 2019)
- Making it an important issue to young Australians
Contributing factors
Top three reasons for discrimination (2020)
- Gender (41.1%)
- Race/cultural background (30.4%)
- Mental health (26%)
Gender differences in reasons
- More than twice the proportion of females than males reported gender as reason (48.0% compared with 22.5%)
- Greater proportion of males than females reported race/cultural background as reason (35.4% compared with 28.8%)
Impact of discrimination
The Scanlon Foundation reports that 2019 survey of social cohesion found just under 25% of young people aged 18 to 24 reported discrimination because of their 'skin colour, ethnic origin or religion'. Most frequent impact was:
- Anger and frustration
- Sense of not belonging to local community
Cultural conflict
Whether born in Australia or overseas, young people from different ethnic backgrounds can feel caught between two sets of cultural standards and values:
- Parents may feel adopting Australian values and customs would risk losing traditional culture
- They may use strict discipline to address perceived permissiveness in Australian society
- Feeling restricted in choice of friends, dating and socialising were major sources of family conflict
- Social isolation can be problem due to language and cultural differences and bullying
Poorer outcomes
For young people from diverse backgrounds:
- Increased risk of suicide
- Risk-taking behaviours
- Increased vulnerability to drug or alcohol problems
- Anxiety
- Depression
- Poor self-esteem
Racism
Racism may affect mental health and wellbeing by:
- Placing less value on individual's identity and sense of self
- Lowering self-esteem and confidence
- Causing people to withdraw from social contact
- Creating fear of going to school or work
- Increasing risk of mental disorders (depression, anxiety, substance use)
Key Points to Remember:
- Youth is a critical transition period where investing in health and wellbeing provides both immediate and long-term benefits for individuals and society
- Health inequalities among young people often result from avoidable sociocultural factors including income, education, and social exclusion, with disadvantaged communities experiencing significantly poorer outcomes
- Eight key areas require health action for Australian youth: injury, alcohol use, illicit drug use, smoking, weight issues, sexual health, stress and mental health, and discrimination
- Risk factors (such as peer pressure, alcohol use, brain development, and social exclusion) interact with protective factors to influence youth health outcomes
- Successful health action requires clear goal setting with specific actions, success indicators, and timelines to replace health-compromising behaviours with health-enhancing behaviours
- The brain continues developing until around age 25, affecting decision-making, impulse control, and risk assessment
- While some trends show positive improvements (decreased smoking, later age of first alcohol use, reduced drug use), other areas remain concerning (mental health, discrimination, obesity)
- Indigenous youth face disproportionate challenges across almost all health areas, experiencing higher rates of injury, substance use, discrimination, and poorer health outcomes