Differences Between Indigenous and Non-Indigenous Population Groups (VCE SSCE Health and Human Development): Revision Notes
Differences Between Indigenous and Non-Indigenous Population Groups
Introduction
Indigenous Australians represent 3.3 per cent of Australia's population and experience significantly poorer health outcomes compared to non-Indigenous Australians across nearly all health indicators. Understanding these disparities requires examining the complex interplay of biological, sociocultural and environmental factors that influence health status.
While Australia's overall life expectancy has increased dramatically from approximately 57 years in 1901 to around 82 years in 2019, these improvements have not been equally shared across the population. Indigenous Australians, along with males, people of low socioeconomic status, and those living outside major cities, continue to experience substantially lower life expectancy than the national average.
Indigenous Australians are defined as Australians of Aboriginal or Torres Strait Islander origin. This term encompasses both Aboriginal peoples and Torres Strait Islander peoples, who have distinct cultures, languages, and histories.
Key differences in health status
Life expectancy and mortality
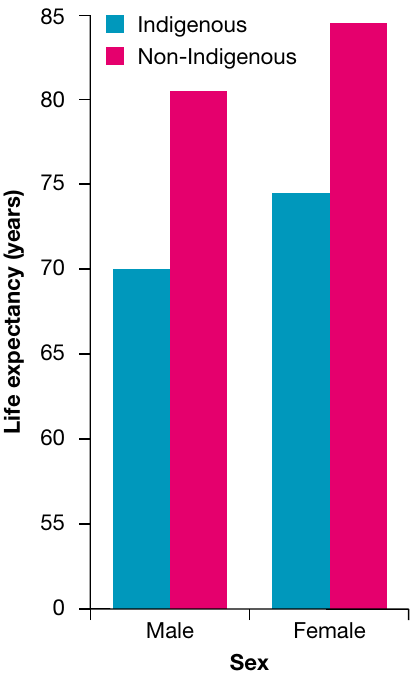
The gap in life expectancy between Indigenous and non-Indigenous Australians remains substantial. In 2017, Indigenous Australians had a life expectancy of 71.6 years for males and 74.6 years for females. This represents a difference of approximately 10.5 years for males and 10.2 years for females when compared with the rest of the population.
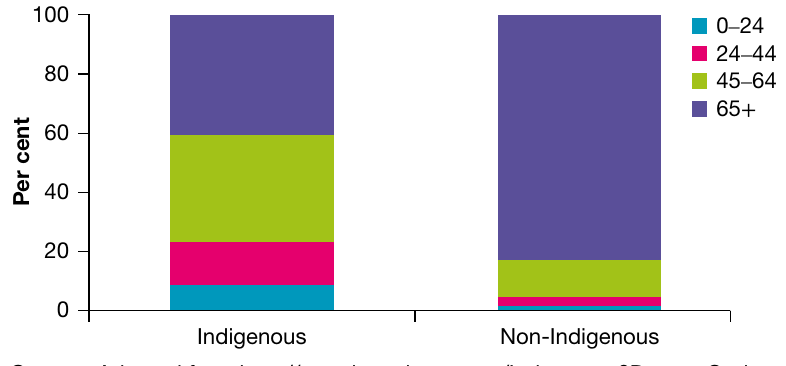
Indigenous Australians face higher mortality rates at every stage of life. Approximately 60 per cent of Indigenous people die before their sixty-fifth birthday, compared to just under 20 per cent for the non-Indigenous population. This demonstrates that Indigenous Australians are not only dying younger, but are more likely to die at every age group.
Comprehensive health status variations
Indigenous Australians experience poorer health outcomes across multiple measures:
Mortality and life expectancy:
- Overall mortality rate almost two times higher than other Australians
- Mortality rate four times higher among Indigenous people aged 35-44
- Infant mortality rates two times higher than the rest of the population
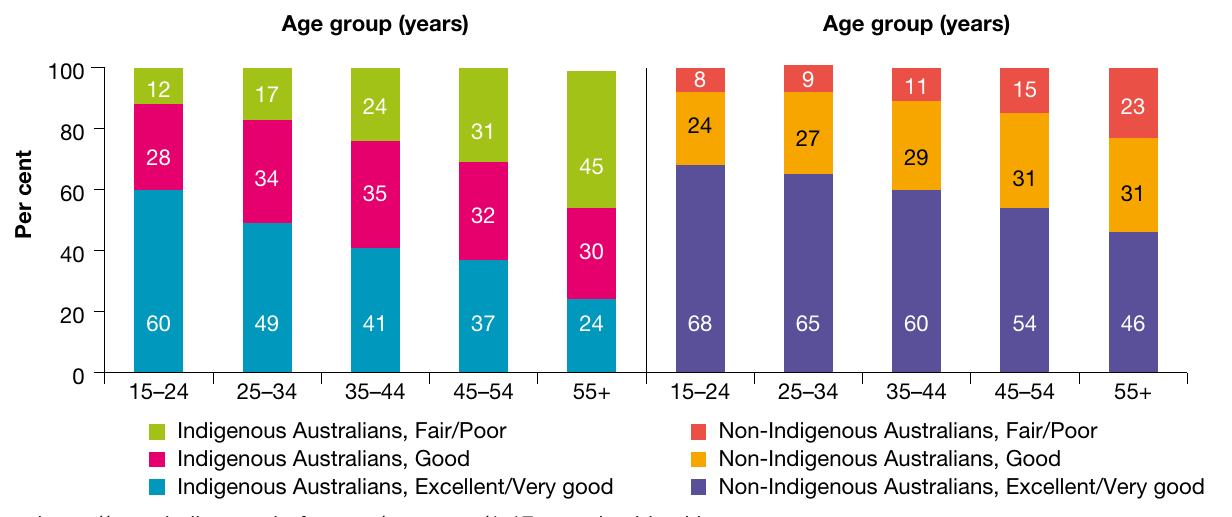
Self-rated health:
- Half as likely to report health status as excellent or very good
- Twice as likely to report health status as fair or poor
Disease burden and chronic conditions:
- Burden of disease 2.3 times the rate of other Australians
- Cardiovascular disease incidence and mortality rates 1.5 times greater
- Cancer mortality rates 1.3 times higher, with significantly higher rates for lung, cervical and liver cancers
- Diabetes and high blood glucose levels more than three times higher, with mortality rates from diabetes five times higher
- Chronic kidney disease rates nearly four times higher
- Respiratory disease burden (including COPD) 2.5 times higher
- Almost twice as likely to report having asthma
Injuries and hospitalisation:
- Hospitalisation and death from injury two times higher
- Higher rates of sexually transmissible infections, with burden from unsafe sexual practices nearly four times higher
Mental health and disability:
- Nearly twice as likely to have a disability or restrictive long-term health condition
- High or very high psychological distress experienced at nearly three times the rate of non-Indigenous population
- Suicide rates four times higher
- Hospitalisation for mental health issues twice as high
Other health conditions:
- Higher rates of dental decay and gum disease
- Indigenous Australians more likely to develop diabetes at a younger age and die from it earlier
Factors contributing to variations in health status
The poorer health status of Indigenous Australians results from a complex interaction of biological, sociocultural and environmental factors. No single factor acts in isolation; rather, these factors work together to create cumulative disadvantage.
Understanding health disparities requires a holistic view that recognizes how biological, sociocultural, and environmental factors interconnect and compound over time. This interconnection means that addressing one factor in isolation is unlikely to produce significant improvements in health outcomes.
Biological factors
Body weight
Aboriginal and Torres Strait Islander peoples experience higher rates of high body mass index across all ages. The obesity rate among Indigenous adults is one and a half times higher than in the non-Indigenous population. Obesity increases the risk of chronic conditions including cardiovascular disease, type 2 diabetes and osteoarthritis.
Being obese is strongly linked to Syndrome X (also called metabolic syndrome), which represents a major health challenge for Indigenous populations.
Syndrome X (Metabolic Syndrome) occurs when a person exhibits a range of factors that increase their risk of cardiovascular disease and type 2 diabetes. These factors include abdominal obesity, high cholesterol and insulin resistance.
This is not a single disease but rather a cluster of conditions that together dramatically increase health risks.
Syndrome X involves the simultaneous occurrence of several unhealthy conditions:
- Abdominal fat accumulation
- Low levels of good cholesterol (high-density lipoprotein or HDL)
- High levels of triglycerides (harmful blood fats)
- High blood pressure
- High blood sugar with high insulin levels, indicating insulin resistance
While Syndrome X is not a disease itself, this collection of conditions dramatically increases the risk of serious health problems.
The consequences of Syndrome X are severe, leading to increased risk of:
- Heart disease (including heart failure and heart attacks)
- Strokes
- High blood pressure
- Type 2 diabetes
- Renal failure requiring dialysis or transplantation
Collectively, these conditions increase the risk of premature death by six times the average rate.
Blood pressure
Indigenous Australians are 1.3 times more likely to report hypertension compared to non-Indigenous Australians. High blood pressure is a significant risk factor for stroke and heart disease.
Glucose regulation
Higher rates of impaired glucose regulation among Indigenous Australians contribute to the elevated rates of diabetes and kidney disease experienced by this population. The body's inability to properly regulate blood sugar levels creates a cascade of health problems.
The connection between glucose regulation and health outcomes is direct: impaired glucose regulation leads to diabetes, which in turn increases the risk of kidney disease, cardiovascular disease, and various other complications. This demonstrates how one biological factor can trigger multiple adverse health outcomes.
Birth weight
Aboriginal and Torres Strait Islander mothers are almost twice as likely to give birth to a baby with low birth weight compared with other Australians. In 2018, 11.7 per cent of live births to Indigenous mothers were classified as low birth weight, compared with 6.4 per cent for non-Indigenous mothers.

Several factors contribute to this disparity:
- Maternal tobacco use
- Poor maternal nutrition
- Limited access to healthcare during pregnancy
Additionally, babies of Indigenous mothers were more likely to be premature, with 14 per cent born prematurely compared to 8.5 per cent for non-Indigenous mothers. Low birth weight and prematurity contribute to higher under-five mortality rates and can affect health throughout life.
Sociocultural factors
Socioeconomic status
Indigenous Australians are more likely to experience lower socioeconomic status than non-Indigenous Australians. On average, Aboriginal and Torres Strait Islander peoples have:
- Lower incomes
- Poorer educational achievements
- Lower rates of home ownership
Lower educational outcomes contribute to reduced levels of health literacy (the ability to understand and use health information). This places Indigenous Australians at greater risk of engaging in harmful behaviours such as smoking, poor dietary choices and sedentary lifestyles. These behaviours further contribute to obesity, type 2 diabetes, cardiovascular disease and lung cancer.
Health literacy is crucial for making informed health decisions. When individuals cannot understand health information, they struggle to:
- Follow medical instructions correctly
- Recognize early warning signs of disease
- Navigate the healthcare system effectively
- Make healthy lifestyle choices
This creates a cycle where lower health literacy leads to poorer health outcomes, which in turn can further reduce opportunities for education and health knowledge.
Unemployment
In 2019, Indigenous Australians were four times as likely to be unemployed as other Australians, with unemployment rates of 19 per cent compared to 5 per cent. Unemployment is even more pronounced for those living outside Australia's major cities, where rates for Aboriginal and Torres Strait Islander peoples range from 20-28 per cent.
Unemployment is strongly associated with various risk factors and poor health outcomes:
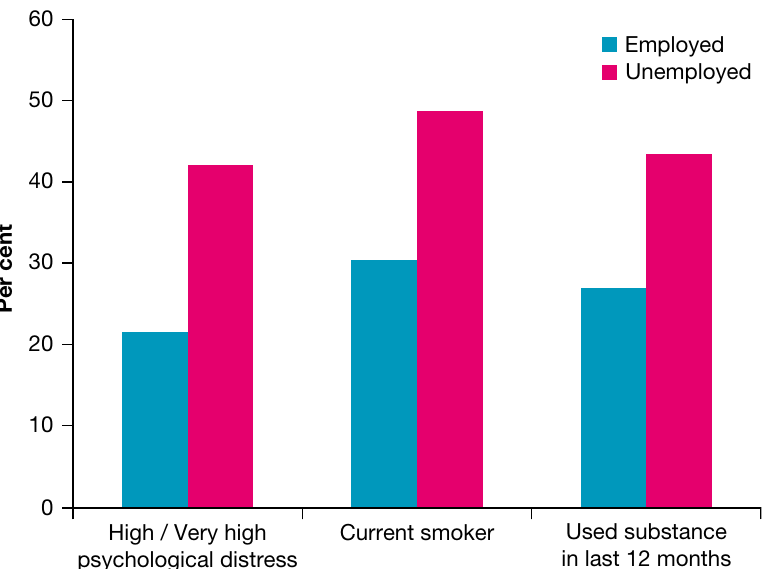
The relationship between unemployment and health includes:
- Increased rates of smoking and alcohol abuse
- Reduced overall feelings of wellbeing
- Higher rates of cardiovascular disease
- Elevated rates of mental health problems
- Increased risk of lung cancer
Unemployment creates a cascade of health risks. Without stable income, individuals face:
- Reduced access to nutritious food
- Inability to afford healthcare and medications
- Increased stress and mental health challenges
- Greater likelihood of engaging in risky behaviours
- Social isolation and reduced sense of purpose
These factors combine to significantly impact both physical and mental health outcomes.
Social exclusion
Social exclusion manifests in several damaging ways for Aboriginal and Torres Strait Islander peoples.
Discrimination and racism:
Discrimination and racism have been directly associated with poorer health status for Aboriginal and Torres Strait Islander peoples, particularly affecting mental health. According to health surveys, 32 per cent of Aboriginal and Torres Strait Islander adults reported avoiding healthcare due to cultural factors including:
- Language barriers
- Lack of trust in health providers
- Experiences of discrimination
This avoidance of healthcare can increase disease duration and severity, contributing to higher morbidity and mortality.
An Aboriginal experience of racism survey conducted in Victoria (2010-11) revealed alarming levels of discrimination:
- Almost all respondents (97 per cent) had experienced at least one racist incident in the preceding 12 months
- Two in three (67 per cent) experienced racism in shops
- 59 per cent experienced racism in public spaces
- 29 per cent experienced racism within health settings
Aboriginal and Torres Strait Islander adults who experienced high levels of racism were significantly more likely to have high or very high levels of psychological distress.
Forced removal from family:
The effects of forced removal continue to impact Indigenous health:
- 17.5 per cent of Aboriginal and Torres Strait Islander adults reported having been removed from their natural family by welfare authorities, government, or by being taken to a mission
- 36 per cent reported that relatives had been removed from their natural family
- In total, more than half (53.5 per cent) reported that either they or their relatives had been removed from their natural family
The trauma of forced removal creates lasting psychological impacts. Levels of high or very high psychological distress were significantly more common among:
- Aboriginal and Torres Strait Islander adults who had been removed from their family (41.2 per cent)
- Those who had relatives removed (36.2 per cent)
- Compared with those who had not experienced removal (26.3 per cent)
High levels of psychological distress increase the rate of risky behaviours such as tobacco and alcohol use and self-harm, raising the risk of cardiovascular disease, respiratory diseases, some cancers and suicide.
Homelessness:
In 2016, an estimated 23,437 Aboriginal and Torres Strait Islander people were experiencing homelessness in Australia—a rate nearly 10 times that of other Australians. Of all homeless people who provided information on their Indigenous status, 20 per cent were Indigenous.
Homelessness increases the risk of:
- Psychological distress
- Risk-taking behaviours including tobacco and alcohol abuse
- Mental health disorders
- Obesity
- Type 2 diabetes
- Cardiovascular disease
- Some cancers
Food insecurity
Aboriginal and Torres Strait Islander peoples are significantly more likely to report food insecurity compared with the general population. Several factors contribute to this disparity:
- Lower incomes
- Poorer quality and overcrowded housing
- Higher cost of fresh foods in areas outside major cities
- Lack of transport
- Lower levels of nutritional knowledge
Food insecurity contributes to higher rates of obesity and associated conditions such as type 2 diabetes, kidney disease and cardiovascular disease.

Traditional Indigenous diets were high in protein and low in fat, providing excellent nutrition. However, European influences have significantly changed dietary patterns for many Aboriginal and Torres Strait Islander peoples, contributing to higher rates of obesity and related conditions.
The shift from traditional diets to Western diets high in processed foods and refined sugars has had profound negative impacts on Indigenous health.
Early life experiences
Maternal substance use during pregnancy has significant impacts on Indigenous health status.
Tobacco use: 44 per cent of Aboriginal and Torres Strait Islander women smoked while pregnant, compared to 10 per cent of other women.
Alcohol use: While national data are limited, some studies suggest that up to 50 per cent of babies born in some Aboriginal and Torres Strait Islander communities display effects of maternal alcohol use.
Drug use: Babies born to Aboriginal and Torres Strait Islander mothers were around 3.5 times more likely to display signs of exposure to drugs while in the uterus.
These differences in substance use during pregnancy contribute to higher rates of:
- Low birth weight babies
- Some infections among infants
- Foetal alcohol spectrum disorder
- Under-five mortality
- Cardiovascular disease
- Type 2 diabetes
Foetal alcohol spectrum disorder is a group of conditions that can occur in a person whose mother drank alcohol during pregnancy. Problems include low birth weight, distinctive facial features, heart defects, behavioural problems and intellectual disability.
Cultural norms
Cultural norms contribute to lower rates at which many Aboriginal and Torres Strait Islander people access western medicine. Many feel western medicine is culturally inappropriate and associate hospitals with death. As a result, many conditions go unchecked for extended periods, which can increase morbidity and mortality rates and reduce life expectancy.
The cultural disconnect between Indigenous peoples and Western healthcare systems is a significant barrier to health service utilization. Addressing this requires:
- Culturally appropriate healthcare services
- Indigenous health workers
- Integration of traditional healing practices where appropriate
- Building trust between Indigenous communities and healthcare providers
Environmental factors
Housing
Housing plays a major role in the health and wellbeing of Aboriginal and Torres Strait Islander peoples. The absence of affordable, secure and appropriate housing can result in homelessness, poor health and wellbeing, and lower rates of employment and education participation, all leading to social exclusion.
Housing quality issues:
Among Aboriginal and Torres Strait Islander households in 2018-19:
- One in three (33 per cent) reported living in a dwelling with one or more major structural problems, such as electrical or plumbing problems, major cracks in floors or walls, or roof defects
- Around one in ten (10 per cent) reported living in a dwelling lacking at least one working facility such as a fridge, cooking facilities, toilet, or bath or shower

These substandard dwellings pose many risks to health status, including increased risk of injury, disease and mental health problems.
Overcrowding:
17.9 per cent of Aboriginal and Torres Strait Islander people were living in overcrowded housing in 2019 compared to 4.9 per cent of other Australians. Overcrowded housing places strain on bathroom, kitchen and laundry facilities, leading to:
- Unhygienic living conditions
- Increased risk of injury
- Higher rates of disease transmission
- Mental health issues
Overcrowded housing creates multiple health hazards:
- Limited personal space increases stress and mental health issues
- Shared facilities become unhygienic more quickly
- Infectious diseases spread more easily in close quarters
- Children lack adequate space for homework and development
- Sleep quality is reduced, affecting overall health and wellbeing
Environmental tobacco smoke:
In 2018-19, Aboriginal and Torres Strait Islander children aged 0-14 were four times as likely as other children to live in households with a daily smoker who smoked indoors (9 per cent compared to 2.1 per cent). Exposure to environmental tobacco smoke:
- Increases risk of respiratory diseases such as asthma
- Can increase the likelihood of children becoming smokers when older
- Is associated with cardiovascular disease
Water and sanitation
While most Australians enjoy one of the cleanest and most reliable water supplies in the world, many Indigenous communities face significant challenges.
Water supply issues:
The 2006 Community housing and infrastructure needs survey found that:
- 48 of 148 Aboriginal and Torres Strait Islander communities tested (about 12,000 people) had drinking water supplies that failed testing at least once in the 12 months before the survey
- Of 82,300 people surveyed, 59 per cent (about 48,500 people) experienced an interruption to their water supply in the previous 12 months
Sewerage problems:
In 2006, 40 per cent of Aboriginal and Torres Strait Islander communities (about 30,000 people) experienced a sewage leak or overflow.
Lack of clean water and adequate sanitation increases the risk of:
- Infectious diseases including gastroenteritis, diarrhoea, dysentery and cholera
- Repeated infections, particularly dangerous for children
- Higher morbidity and mortality rates
- Dental decay (due to lack of fluoridated water supply in many areas)
Access to clean water and proper sanitation is a fundamental human right and a basic requirement for health. The fact that significant numbers of Indigenous Australians lack these basics in a developed nation like Australia represents a critical health equity issue.
Access to health services
Indigenous Australians have lower levels of access to and use of health services and resources, including:
- Medicare-funded services
- Pharmaceutical Benefits Scheme (PBS), which subsidises medication
- Private general practitioners
Approximately 21 per cent of Aboriginal and Torres Strait Islander people live in remote areas, compared to 2 per cent of the rest of the population. This geographic isolation makes service delivery and access to services more difficult. As a result:
- Conditions may go undiagnosed or untreated
- Treatment options may be limited
- Morbidity and mortality rates increase
Geographic isolation creates a compound barrier to healthcare. Remote communities face:
- Fewer healthcare facilities and professionals
- Greater distances to travel for medical care
- Higher costs associated with accessing services
- Delayed treatment due to distance
- Limited specialist services
- Reduced access to preventive care and health screening programs
These factors mean that by the time Indigenous Australians in remote areas receive medical attention, conditions are often more advanced and harder to treat.
Infrastructure
Aboriginal and Torres Strait Islander people living outside Australia's major cities face additional environmental challenges:
- Unsealed roads
- Poorer lighting at night
- Increased risk of injuries and deaths from road crashes
Summary of contributing factors
The health disparities experienced by Indigenous Australians result from the complex interaction of multiple factors across biological, sociocultural and environmental domains. These factors do not operate independently but rather create cumulative disadvantage that compounds over time and across generations.
Understanding the interconnected nature of these factors is crucial. For example:
- Low socioeconomic status leads to poor housing conditions
- Poor housing conditions contribute to higher rates of infectious disease
- Infectious diseases in childhood can affect development and education
- Lower educational outcomes reduce employment opportunities
- Unemployment perpetuates low socioeconomic status
This cycle demonstrates how factors in one domain (sociocultural) directly impact factors in another (environmental), which then affect biological outcomes, creating a self-reinforcing cycle of disadvantage.
Understanding these interconnected factors is essential for developing effective strategies to address health inequalities and improve health outcomes for Aboriginal and Torres Strait Islander peoples.
Remember!
Key Points to Remember:
-
Indigenous Australians experience a life expectancy gap of approximately 10 years compared to non-Indigenous Australians, with higher mortality rates at every age group.
-
Biological factors including high BMI, hypertension, impaired glucose regulation and low birth weight contribute to higher rates of chronic diseases, particularly Syndrome X, which increases premature death risk by six times.
-
Sociocultural factors create cumulative disadvantage through low socioeconomic status, unemployment rates four times higher than the general population, social exclusion (including discrimination, forced removal from families and homelessness), food insecurity and culturally inappropriate healthcare.
-
Environmental factors including substandard and overcrowded housing, inadequate water and sanitation systems, limited healthcare access (particularly in remote areas) and poor infrastructure create additional health risks.
-
These biological, sociocultural and environmental factors interact in complex ways rather than operating in isolation, creating a cycle of disadvantage that requires comprehensive, multi-faceted approaches to address health inequalities.