The Role of Episodic and Semantic Memory (VCE SSCE Psychology): Revision Notes
The Role of Episodic and Semantic Memory
Introduction
People vary in how vividly they can visualise mental images. Research from the University of New South Wales found that individuals with aphantasia (inability to visualise images) showed reduced fear responses when reading scary scenarios. This demonstrates a link between mental imagery and emotions, with imagery acting as an 'emotional thought amplifier'. This finding highlights the importance of visual imagery in memory and emotional processing.
This groundbreaking research reveals that the vividness of our mental imagery directly influences the intensity of our emotional responses. People who cannot visualise images experience significantly weaker emotional reactions to imagined scenarios, demonstrating that mental imagery serves as a powerful amplifier for our emotions.
What are episodic and semantic memories?
Semantic memory
Semantic memory refers to organised factual knowledge about the world. This includes general information that can be researched and verified, such as capital cities, scientific formulas, or historical facts. Examples include:
- The capital of Norway
- The main ingredient in an omelette
- The animals on an Australian 50-cent coin
- The colour of a $20 note
Semantic memories are impersonal and objective. Different people should arrive at the same answer when recalling semantic information.
Think of semantic memory as a mental encyclopedia or database. It contains facts and knowledge that exist independently of your personal experiences. When you recall that Paris is the capital of France, you're accessing semantic memory – this fact is the same for everyone, regardless of whether you've visited Paris or not.
Episodic memory
Episodic memory stores personal experiences and events that occurred at specific times and places. These memories function like a personal diary, recording distinct episodes from our lives. Examples include:
- Your 10th birthday party
- An accident you witnessed
- Your first day at secondary school
- What you did last weekend

Episodic memories are typically more easily forgotten than semantic memories. This occurs because new personal experiences constantly enter episodic memory, making it difficult to attend to, encode and store each new event.
Why are episodic memories more fragile?
Unlike semantic memories, which are reinforced through repeated exposure and use, episodic memories are often experienced only once. The constant influx of new personal experiences creates competition for attention and storage resources in our memory system, making individual episodes more vulnerable to being forgotten.
Key differences
Episodic memories are personal and context-dependent, linked to specific times and places. Semantic memories are factual and impersonal, consisting of general knowledge that exists independently of personal experience. However, these two memory systems often work together rather than operating in complete isolation.
The role of episodic and semantic memory in retrieving and constructing events
Retrieving autobiographical events from the past
Episodic and semantic memories interact to form autobiographical memories. Autobiographical memory is a memory system consisting of episodes from a person's life, combining both episodic elements (sensory details, emotions, temporal and spatial context) and semantic elements (general knowledge, personal facts without specific context).
Example: A Student Studying for an Assignment
Consider a student studying for an assignment. The memory of this event would include:
Episodic elements:
- Where they studied (the library, their bedroom)
- When they started and finished
- Interruptions from friends
Semantic elements:
- New information learned about the topic
- Facts acquired during research
- Concepts and theories understood
Autobiographical memory functions as more than just episodic memory. It represents a constructive and integrative information processing system. An important function is supporting our sense of self and identity. Our self-identity includes:
- Abstract representations of personal characteristics (traits like "I am timid")
- General knowledge about life periods ("When I was in primary school, we visited grandma on Sundays")
- Specific past events ("The time I broke my leg in grandma's garden")
Whilst episodic memories are individual past events, autobiographical memory links these events together into a personal history connecting self through past, present and future, forming a life narrative.
Reconstruction of memories
When retrieving autobiographical experiences, we use reconstruction. This involves combining stored information with other available information to form what we believe to be a more coherent, complete or accurate memory.
Example: Recalling a Favourite Holiday
When recalling a favourite holiday, you might remember where you went, who was present, what you wore and what happened. These features and events are recalled from different locations in long-term memory and pieced together like a jigsaw puzzle.

Memory is Not a Perfect Recording
This reconstruction process means memory retrieval is not always accurate. We tend to include information that was not part of the original experience, filling gaps or unconsciously altering events to make them more sensible to us. Your memories are actively constructed each time you recall them, not played back like a video recording.
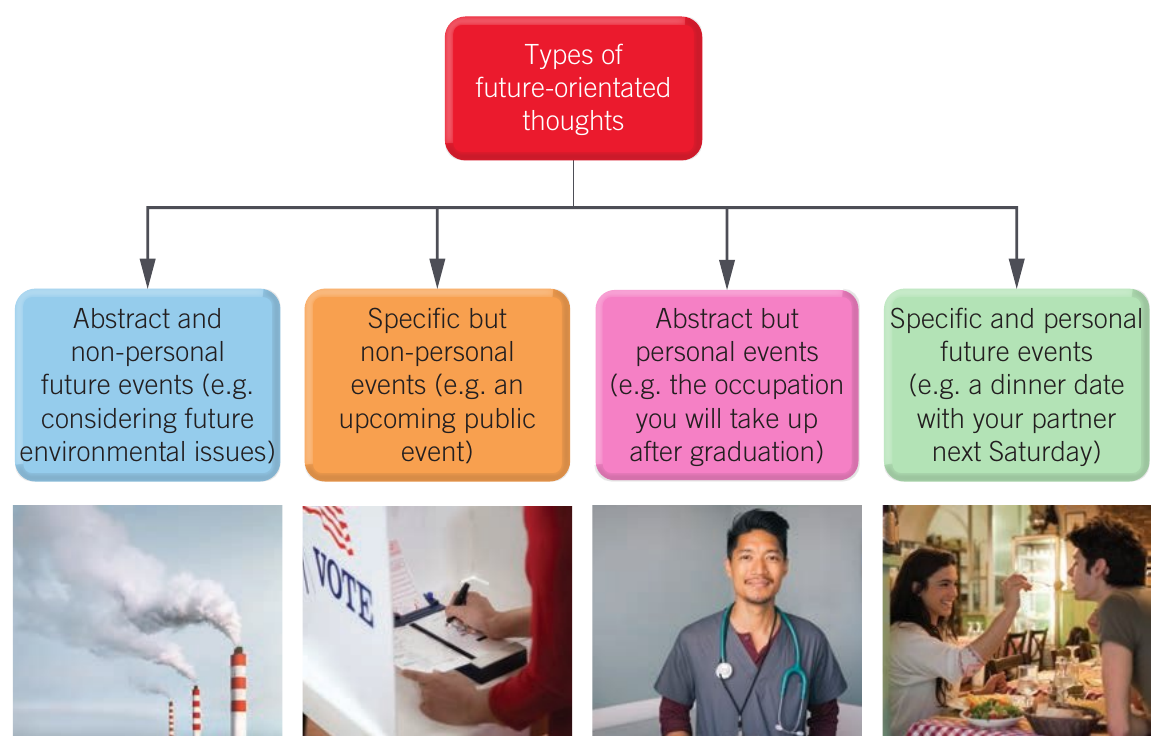
Constructing possible imagined futures
Recent research suggests episodic and semantic memory also enable us to imagine and envision possible future scenarios. This ability is called episodic future thinking or mental time travel. It involves projecting yourself forwards in time to pre-experience events that might happen in your personal future.
Researchers discovered that autobiographical memories and episodic future thinking occur in the same brain regions and use similar underlying processes. Evidence came from observing patients with amnesia, who were unable to access autobiographical memories and also could not imagine future events. Functional MRI studies of healthy individuals showed overlapping brain activity when remembering the past and predicting the future.
This remarkable finding challenges the traditional view that memory only serves to record the past. Instead, it reveals that our memory systems evolved not just to store what happened, but to help us simulate what might happen, enabling better planning and decision-making for the future.
The construction process
Episodic future thinking involves active construction of events that have not yet occurred, based on past events and knowledge:
- Episodic memory provides the specific elements (people, objects, locations) used to construct future events and scenarios
- Semantic memory provides the context or framework for constructing and organising episodic future thinking, plus complementary knowledge about personal past
Example: Imagining a Trip to Paris
Semantic memory provides the context:
- Where Paris is located
- What language is spoken
- How to get there
- General facts about landmarks and culture
Episodic memory provides specific details:
- Friends you might meet (based on past social experiences)
- Places you might revisit (if you've been before)
- Specific dishes you might enjoy (based on previous meals)
Similarly, imagining a future wedding involves selecting elements from weddings previously attended, seen on television, in films or magazines.
Evolutionary advantage
The ability to accurately imagine the future provides an evolutionary advantage. Creating detailed simulations of potential futures (university, desired jobs, having children) allows mental exploration of various steps and consideration of potential obstacles. This ability to act with specific, individually anticipated future events in mind may explain why human behaviour is so flexible.
Mental Time Travel as a Survival Tool
Our ancestors who could better imagine future scenarios – such as predicting seasonal changes, planning hunting strategies, or anticipating dangers – were more likely to survive and pass on their genes. This cognitive ability to simulate the future remains one of humanity's most powerful adaptive advantages.
Alzheimer's disease
Historical background
In 1901, Auguste Deter was institutionalised due to unwarranted jealousy towards her husband, memory impairment and disorientation. Dr Alois Alzheimer, a German psychiatrist, observed and recorded her symptoms. Auguste could not remember objects shown to her after brief periods, experienced confusing speech and woke screaming at night.
After Auguste's death at age 55 in 1906, Alzheimer performed an autopsy. He discovered abnormalities and extensive atrophy (shrinkage) in the cortex. Whilst such findings were common in patients in their 70s, Auguste's age made them remarkable. The disorder was subsequently named Alzheimer's disease.
Definition and prevalence
Alzheimer's disease is a neurodegenerative disease characterised by progressive deterioration of brain neurons, causing memory loss, decline in cognitive and social skills and personality changes. It is the most common form of dementia, affecting approximately 70% of people diagnosed with dementia. It typically begins in older age, affecting about 3% of people aged 65-74 years and 32% of people over 85 years. Rare inheritable forms can begin as early as the 30s.
Alzheimer's disease is incurable, with most people dying within 8-10 years of onset. Early detection and intervention can help manage symptoms and improve quality of life, but there is currently no treatment that can stop or reverse the progression of the disease.
Diagnosis
No simple diagnostic test exists for Alzheimer's disease. Brain scans can assist diagnosis by examining brain activity and tissues. Computed tomography (CT) or magnetic resonance imaging (MRI) scans are typically included in standard evaluation. These scans:
- Reveal the anatomic structure of the brain
- Rule out problems such as tumours, haemorrhage or stroke
- Show loss of brain mass in middle or later disease stages
Positron emission tomography (PET) and single-photon emission computed tomography may be performed if CT and MRI scans are inconclusive. These techniques provide images of brain activity based on blood flow, oxygen consumption or glucose use, helping narrow diagnosis by revealing neural abnormalities.
Limitation of Current Diagnostic Methods
Even advanced brain scans cannot show the microscopic lesions (areas of abnormal tissue) in brain tissue that characterise Alzheimer's disease. Definitive diagnosis can only be confirmed through post-mortem examination of brain tissue, making it impossible to be completely certain while the patient is alive.
Symptoms and progression
Alzheimer's disease typically progresses slowly through three general stages: early (2-4 years), middle (2-10 years) and late (1-3 years). Progression varies between individuals. General symptoms include gradual severe memory loss, confusion, impaired attention, disordered thinking, decline in social skills and personality changes.
Initially, patients have impaired explicit memory (episodic and semantic memory). Eventually, both explicit and implicit memory severely decline.
| Early stage (2-4 years) | Middle stage (2-10 years) | Late stage (1-3 years) |
|---|---|---|
| Forgets recently read material | Experiences delusions, compulsions or repetitive behaviour | Has personality and behaviour changes |
| Has trouble organising or planning | Experiences agitation, restlessness and anxiety | Loses ability to hold conversation |
| Forgets where valuables have been placed | Needs assistance with getting dressed | Has difficulty moving, eating and swallowing |
| Has trouble managing money | Bladder and bowel function issues | Loses bladder and bowel control |
| Forgets recent events, names, details about own identity and dates | Has trouble learning new things | Lacks awareness of recent activities or surroundings |
| Has trouble with challenging tasks at work | Has problems with reading and writing | Cannot remember family members and loved ones |
| Becomes lost in familiar places | Loses track of time or surroundings | |
| Experiences sleep disturbances |
Biological causes
Four changes in the brain characterise Alzheimer's disease:
1. Amyloid plaques: Abnormal build-up of beta-amyloid proteins between neuron synapses, interfering with neural communication
2. Neurofibrillary tangles: Protein build-up inside neurons associated with cell death, disrupting information flow within and between neurons
3. Acetylcholine deficiency: Systematic destruction of neurons producing this important memory neurotransmitter
4. Brain atrophy: Progressive neuron damage and death from amyloid plaques and neurofibrillary tangles, causing brain tissue shrinkage
Understanding the Biological Cascade
These four changes don't occur in isolation – they interact and reinforce each other in a devastating cascade. Amyloid plaques and neurofibrillary tangles trigger inflammation and oxidative stress, which accelerate neuron death. The loss of acetylcholine-producing neurons further impairs the brain's ability to form and retrieve memories. This progressive damage eventually leads to widespread brain atrophy.
Progressive damage pattern
The hippocampus is one of the first structures affected by atrophy. Up to three-quarters of neurons die and the rest are damaged. This prevents encoding and consolidation of new explicit memories, resulting in anterograde amnesia (inability to form new explicit long-term memories after the disease onset). For example, individuals cannot learn new things or remember where they placed objects.
Neuron loss then spreads to the cerebral cortex, resulting in:
- Loss of stored explicit long-term memories (episodic, semantic and autobiographical) - retrograde amnesia (inability to retrieve previously stored memories)
- Problems with attention
- Changes to personality and emotions
Example: The Impact of Progressive Damage
In early stages, a person might forget where they placed their keys (anterograde amnesia) but can still remember their childhood and recognize family members.
As the disease progresses, they begin losing older memories too (retrograde amnesia). They might not recognise their adult children or remember significant life events. Personality changes emerge – someone who was always calm might have emotional outbursts.
When autobiographical memories are lost, the capacity for episodic future thinking is also lost. Individuals cannot imagine going on trips or to the supermarket, creating difficulties planning for future events.
Finally, damage extends to the hindbrain (rear of the cortex), which regulates automatic functions such as breathing and heart rate. When hindbrain neurons degenerate in final stages, death occurs.
Aphantasia
Definition and characteristics
Aphantasia is the inability to visualise imagery. The term comes from the ancient Greek word 'phantasia' (imagination) with the prefix 'a-' (without). People with aphantasia have no 'mind's eye' or essentially blind imagination.

Whilst most people can conjure images of scenes or faces in their minds, 2-5% of the population cannot visualise any type of image in their head. When asked to imagine something, individuals with aphantasia can probably describe the object, explain the concept and list facts they know about it, but they cannot experience any mental image accompanying this knowledge.
What Do People with Aphantasia Experience?
Imagine being asked to picture a red apple. Most people will "see" an apple in their mind – its colour, shape, and perhaps even texture. Someone with aphantasia knows what an apple looks like, can describe it perfectly, and recognise one when they see it, but they experience no internal visual representation. Their knowledge exists without the accompanying mental picture.
Impact on daily life
People with aphantasia may:
- Struggle to remember or 'relive' autobiographical events
- Have difficulty imagining future or hypothetical events
- Have problems with factual memory
- Dream less
- Have decreased imagery involving other senses such as sound or touch
- Have trouble recognising faces
- Have trouble remembering everyday things, like the number of windows on a building
Historical context
The first modern account of aphantasia dates to an 1880 study in the United Kingdom, when Sir Francis Galton reported that some men in a group of 100 were unable to create a mental image of their breakfast table. Much current information stems from a few small studies and anecdotal accounts.

Dr Adam Zeman's 2005 case study of patient 'MX' has been important for continuing research. MX lost his ability to generate mental pictures after a simple surgical operation, representing a case of acquired aphantasia.
Causes
Scientists are not certain what causes aphantasia. Suggested explanations include:
- Areas of the brain involved in visual imagery, such as the visual cortex, may be underactive
- People with aphantasia may experience mental imagery but cannot access the image in conscious thoughts
There are two forms of aphantasia:
1. Congenital aphantasia: Present from birth
2. Acquired aphantasia: Develops after brain injury or significant psychological event (such as depression or anxiety)
A 2020 study followed a former architect who developed aphantasia after a stroke affected blood flow to the occipital lobe. This case demonstrates that aphantasia can occur suddenly when specific brain regions involved in visual processing are damaged, providing valuable insights into the neural basis of mental imagery.
Treatment and prognosis
No known 'cure' exists for congenital aphantasia. Some people with acquired aphantasia have reported regaining imagery abilities after undergoing therapy.
Aphantasia is Not a Disability
Importantly, aphantasia is not a disability but rather a unique variation in human experience. Available studies suggest having aphantasia does not necessarily inhibit success in life. Many people with different occupations experience aphantasia, including successful doctorate students, engineers and other professionals. People with aphantasia may not even know they experience the world differently and lead normal lives.
Notable examples include Blake Ross (creator of Mozilla Firefox) and Ed Catmull (co-founder of Pixar and former president of Walt Disney Animation Studios).
Remember!
Key Points to Remember:
-
Episodic memory stores personal experiences linked to specific times and places, whilst semantic memory contains factual knowledge about the world
-
Autobiographical memory combines episodic and semantic elements to form a personal life narrative that supports our sense of self and identity
-
Both memory types work together through reconstruction to retrieve past events and through episodic future thinking to imagine possible futures, providing evolutionary advantages for planning and flexible behaviour
-
Alzheimer's disease progressively destroys memory through biological changes (amyloid plaques, neurofibrillary tangles, acetylcholine deficiency, brain atrophy), causing both anterograde amnesia (inability to form new memories) and retrograde amnesia (loss of stored memories)
-
Aphantasia is the inability to visualise mental imagery, affecting 2-5% of the population. It can be congenital or acquired, impacts memory and imagination, but does not necessarily inhibit success in life