Case Study: Malaria (AQA A-Level Geography): Revision Notes
Case Study: Malaria
What is malaria?
Malaria is a tropical disease transmitted biologically through insect vectors. The disease has a devastating impact on people's health and their livelihoods across the world.
The disease is caused by a single-celled parasite from the Plasmodium family. When a female Anopheles mosquito bites a person, the parasite can be transferred into their bloodstream. Once inside, the parasites multiply in the liver before infecting red blood cells.
The malaria transmission cycle requires both the mosquito vector and the Plasmodium parasite to complete. The parasite undergoes different developmental stages in both the mosquito and human hosts, making the disease complex to control.
Symptoms and progression
The disease manifests through several characteristic symptoms:
- Fever
- Headache
- Vomiting
These symptoms typically appear 10-15 days after the mosquito bite. If malaria is not treated, it can rapidly become life-threatening by disrupting blood supply to vital organs. The disease can either kill a person directly or weaken their immune system, making them vulnerable to other illnesses.
Vector-borne disease
A vector-borne disease is one that is biologically transmitted by insects, which carry the pathogen from one host to another. This biological transmission distinguishes malaria from other diseases and is crucial to understanding how it spreads.
Global distribution and prevalence
Although malaria was once common in many more places around the world, it has been eliminated in numerous populous regions over the course of the twentieth century, including many parts of the USA and Europe. This has saved millions of lives.
Current global statistics (WHO, 2018)
- 3.6 billion people (nearly half the world's population) across 91 countries live in areas at risk of malaria transmission
- An estimated 228 million cases occurred, resulting in around 405,000 deaths
- Children under five years of age are the most vulnerable group, accounting for 67% (272,000) of all malaria deaths worldwide
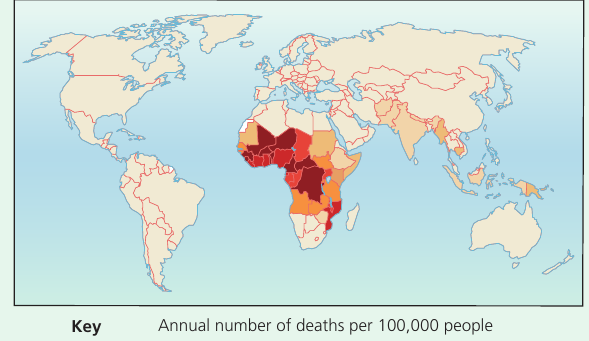
Geographic concentration
Sub-Saharan Africa carries a disproportionately high share of the global malaria burden. In 2018:
- The region was home to 93% of malaria cases
- It accounted for 94% of malaria deaths
The concentration of malaria cases in Sub-Saharan Africa reflects a combination of environmental factors (favorable climate for mosquito breeding), socio-economic conditions (poverty and limited healthcare infrastructure), and biological factors (presence of the most deadly Plasmodium species).
Countries most affected
Specific countries bear the heaviest burden:
- 19 countries in sub-Saharan Africa plus India carried almost 85% of the global malaria burden
- Six countries accounted for more than half of all malaria deaths worldwide:
- Nigeria (25%)
- Democratic Republic of the Congo (12%)
- Uganda (5%)
- Côte d'Ivoire, Mozambique and Niger (4% each)
Environmental factors influencing malaria transmission
Physical environment and seasonal patterns
Malaria is strongly linked to the natural environment. The transmission of the disease is greatest in areas where both the rainy season and temperatures are suitable for mosquito breeding.
Mosquitoes breed in stagnant water, which means transmission is enhanced in areas with standing water after the rainy season. The length of the malaria transmission season is directly related to the length of the rainy season.
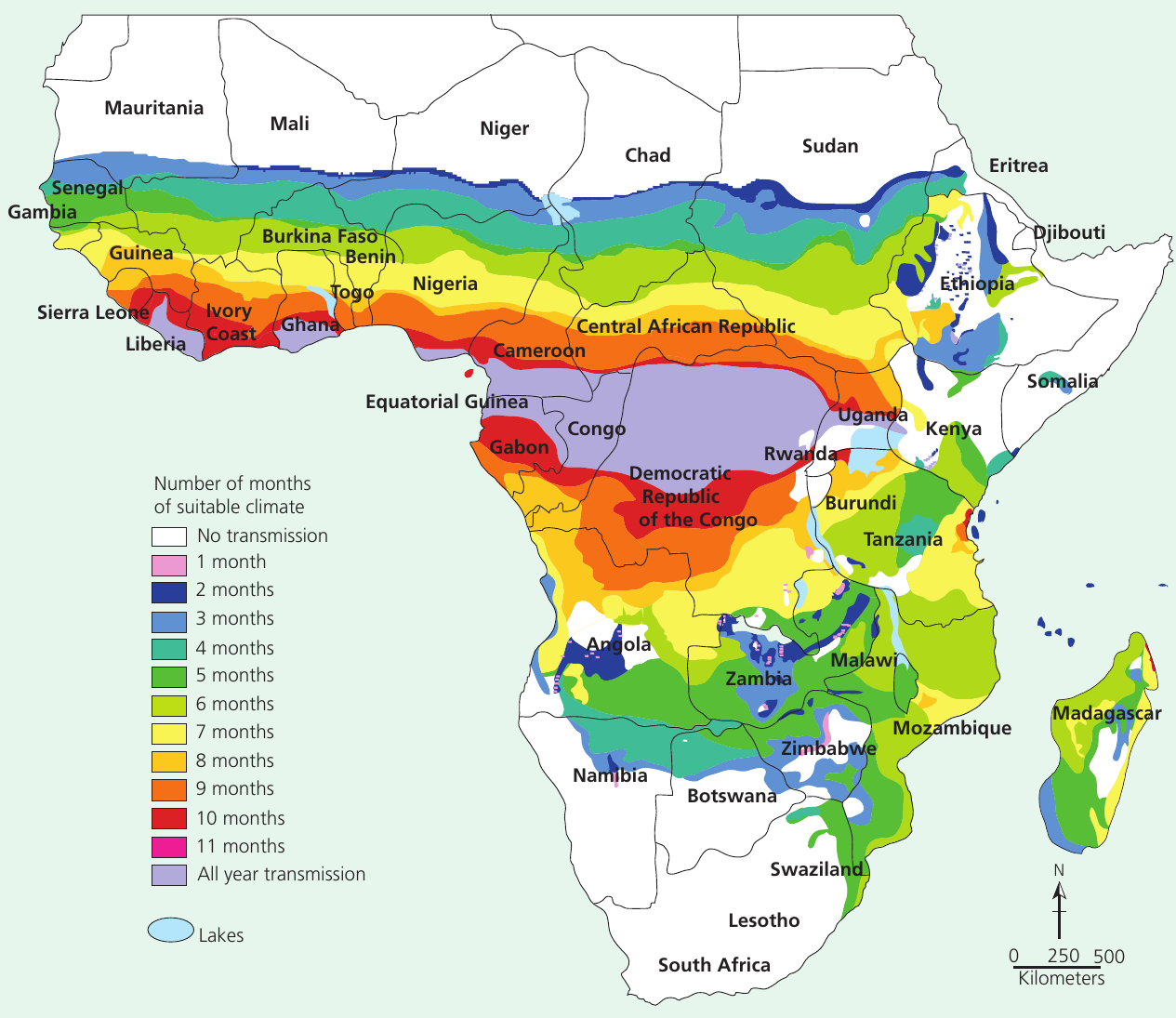
Temperature requirements
Temperature plays a crucial role in malaria transmission:
- At altitudes above 1,500m and where rainfall is below 1,000mm, malaria transmissions fall
- The parasites require temperatures between 16°C and 32°C to develop inside the mosquito
- This is one reason why the disease is largely concentrated in the tropics and subtropics
The temperature range of to is critical because the Plasmodium parasite cannot complete its life cycle in the mosquito at temperatures outside this range. This is why malaria is rare in temperate climates and at high altitudes, even in tropical regions.
Altitude and rainfall patterns
Areas at high altitude with low rainfall typically experience reduced transmission. This is because cooler temperatures at higher elevations fall outside the optimal range for parasite development.
Seasonal variations
Climate change will gradually alter the pattern of the transmission season in all areas over time:
- Areas receiving more flood events may show higher incidence of transmission over a longer period
- Regions that become more prone to drought may have shorter transmission seasons but will face other health challenges
Climate change is expected to alter malaria distribution patterns globally. Some areas may see increased transmission due to warming temperatures and changing rainfall patterns, while others may experience reduced transmission. This makes long-term planning for malaria control more challenging.
Coastal areas
On a smaller scale, coastal areas have much less seasonal variation in temperature. These areas are:
- Lower in altitude
- Have higher relative humidity
- Temperatures lie within the transmission vector's range of tolerance
This means coastal areas often show a higher prevalence of the disease throughout the year.
Land use factors
Land use is another important factor determining malaria risk. Studies in India have shown that those living in proximity to forested areas (with higher humidity) are more susceptible to infection.
Socio-economic factors influencing malaria risk
While environmental variables are the overriding determinant of malarial mosquito presence, socio-economic factors also influence the level of risk of contracting the disease. Malaria is often referred to as a disease of poverty.
Disability adjusted life years (DALYs)
When the burden of malaria is measured as disability adjusted life years (DALYs), nearly two-thirds of the total global burden due to malaria is concentrated among the poorest 20% of the world's population. This metric accounts for both years of life lost to premature death and years lived with disability.
Malaria is a common cause of morbidity in many countries but is concentrated in the world's poorest continents. This is due to the lack of investment in projects for developing new drugs and vaccines, and the limited availability of existing programmes to control the disease.
Studies undertaken in Africa, Asia and South America have identified a number of prevailing socio-economic variables that increase the incidence of malarial infection:
Poor housing quality
Homes with earth or sand floors using materials such as mud, bamboo cane or wooden trunks for walls, and grass or palm leaves to provide a roof face higher risk. Those with:
- Poorly-fitted windows or doors
- Windows without glass, screens, curtains or shutters
are particularly vulnerable to mosquito entry.
Housing quality is one of the most significant socio-economic risk factors for malaria. Poor housing construction allows mosquitoes easy access to residents during sleeping hours when people are most vulnerable to bites. Simple improvements like fitted screens can dramatically reduce exposure.
High density occupancy
Densely clustered built-up areas and overcrowded rooms (for sleeping) represent another important risk factor. High malaria incidence is associated with:
- High infant mortality rates
- Subsequently high fertility rates
A consequence is that children (and sometimes parents) often share a room with at least five occupants.
Unsanitary conditions
Studies of malaria 'hotspots' in Chennai identified that although individual houses were clean, surrounding areas were dirty and polluted by:
- Rubbish and waste outflows
- Spitting and open defecation
These practices are also commonly associated with attracting mosquitoes.
Occupation
Agricultural workers are more exposed to the mosquito vector. This particularly applies to:
- Those living near to stores of irrigation water
- Migrant workers who may sleep outdoors at night
Case Study: Ethiopian Highland Farmers
Studies in Ethiopia have shown that highland farmers, who seasonally migrate to find work in lowland areas, are particularly prone to malarial infection. These workers move from malaria-free highland areas (above 1,500m) to lowland agricultural regions during harvest season, where they:
- Lack immunity to malaria
- Often sleep outdoors or in temporary shelters
- Work near irrigation systems with standing water
- Cannot afford preventative measures like bed nets
This seasonal migration pattern creates a high-risk population that requires targeted intervention strategies.
Rural vs urban environments
Generally, those in rural areas are seen to be more at risk. However, contamination rates in urban slums and poorer settlements are high due to:
- Building density
- Unsanitary conditions
- Stagnant water being retained in rubbish
Age and gender
These are not significantly associated with the risk of infection, though children aged under 5 are more likely to suffer the extreme consequences of the disease. However, studies in both The Gambia and Tanzania indicate a shift in malaria burden from the under-fives to older children aged 5 to 14 years. This is thought to be as a result of the focus on prevention in the younger age groups through better education, awareness and provision of nets.
Poverty and prevention
It is important to distinguish between the overall risk of infection (determined by the mix of physical and socio-economic environmental factors listed above) and the utilisation of prevention and treatment methods. These have a much clearer association with poverty and socio-economic status, such as the level of income and educational attainment, as well as accessibility to intervention methods.
There is more convincing evidence that vulnerability to the consequences of malaria is higher among lower socio-economic groups:
Income
There is a strong positive correlation between income and the use of prevention methods. Those with higher incomes spend more on:
- Repellents
- Insecticide-treated nets (ITNs)
- Mosquito coils
This reduces their risk of infection. Higher income is associated with better nourishment, and studies show that cerebral malaria is less common in well-nourished children. This disproportionately affects agricultural workers, many of whom receive seasonal incomes at harvest time and cannot afford nets or treatment during the main malaria season.
Education
Those with a clearer understanding of the link between malaria and surrounding environmental conditions (including hygiene and sanitation) are more likely to use prevention strategies. For example, studies in Malawi found that net ownership was largely absent in homes where the head of the household had not completed primary education.
Distance and accessibility
Greater distance to the nearest clinics or hospitals is associated with:
- Fewer people seeking treatment for symptoms
- Less expenditure on prevention methods
For example, repellents and coils are less available and so used less in rural areas. Instead, there is a reliance on burning medicinal plants as a repellent.
The poverty-malaria connection
Most of the variables listed are proxies for poverty. The evidence suggests that malaria infection, and particularly death resulting from malaria, is strongly associated with low socio-economic status. It is children from the poorest income groups living in poor housing who are most at risk.
The relationship between poverty and malaria creates a vicious cycle: poverty increases malaria risk, and malaria perpetuates poverty by reducing productivity, increasing healthcare costs, and limiting economic development. Breaking this cycle requires both disease control measures and broader socio-economic development initiatives.
Impacts of malaria
Health and well-being impacts
Well-being
Well-being can be defined as 'the state of being comfortable, healthy or happy'. Clearly if an individual is ill then they cannot be any of those things. If groups of people are ill, then this has an effect on the economic well-being of a community.
Mortality statistics
Malaria kills a child somewhere in the world every two minutes. Ninety-four per cent of malaria deaths occur in Africa, where malaria accounts for about one in six of all childhood deaths.
Symptoms and disease progression
Malaria causes the patient to develop a high fever, which comes and goes. The pattern of fevers varies according to the species of malaria. Initially, it feels like the flu: high fever, fatigue, and body aches, with hot and cold stages.
Signs and symptoms in children may be nonspecific, leading to delays in diagnosis. People also may have:
- Headache
- Nausea
- Shaking chills (rigors)
- Sweating
- Weakness
Anaemia is common in patients with malaria, partly due to the effects of the Plasmodium parasite on the red cells.
Severe malaria (Plasmodium falciparum)
Plasmodium falciparum causes a particularly severe form of malaria. In addition to fever, patients may experience complications such as:
- Destruction of red blood cells
- Yellow skin discolouration
- Kidney failure
- Fluid in the lungs
- Cerebral malaria
- Convulsions
- Coma
- Death
Plasmodium falciparum is responsible for the majority of malaria deaths worldwide. It can cause severe complications within hours of symptom onset, making early diagnosis and treatment critical. Unlike other malaria species, P. falciparum can affect multiple organs simultaneously and is the primary target of most vaccine development efforts.
Partial immunity
People who have lived for years in areas with malaria may develop a partial immunity to new infections.
Impacts on women and children
The disease also contributes greatly to anaemia among women and children. Infection during pregnancy is associated with:
- Severe anaemia and other illness in the mother
- Low birth weight among newborn babies (one of the leading risk factors for infant mortality)
- Sub-optimal growth and development
Economic impacts
Malaria has serious and far-reaching impacts, slowing economic growth and development and prolonging the vicious cycle of poverty. While it is true that poverty and lack of development may be key causes of the presence of malaria, there is a strong argument that malaria causes underdevelopment.
Costs to individuals and families
These include:
- Travel to and treatment at clinics
- Purchase of drugs to treat malaria
- Lost income from absence from work
- Reduction in crop production
- Absence from school
- Purchase of preventative measures
- Burial expenses in cases of death
Costs to government
Government expenditure includes:
- Building, staffing and maintaining healthcare facilities
- Purchase of drugs and public health intervention equipment such as insecticides and nets
- Loss of production and revenue from taxes during absences
- Loss of tourism revenue
Healthcare burden statistics
It has been estimated that in many parts of west and central Africa, malaria accounts for:
- Up to 40% of public health expenditure
- 30-50% of inpatient hospital admissions
- 60% of outpatient hospital clinic visits
These statistics reveal the enormous strain malaria places on already underfunded healthcare systems in affected countries. The resources devoted to malaria treatment and prevention represent opportunity costs - funds and personnel that could otherwise address other health priorities.
Direct and indirect costs
The direct costs of malaria resulting from the provision of healthcare are thought to be around US$15-18 billion each year globally. In addition, there are many indirect costs resulting from:
- Lost economic growth
- Lost productivity
- The lack of foreign investment in industry, commerce or tourism
Management and mitigation strategies
Elimination vs Eradication
Malaria elimination is defined as the interruption of local transmission of the Plasmodium parasite species in a defined geographical area as a result of deliberate intervention (WHO).
Eradication, however, is defined as the permanent reduction to zero of the worldwide incidence of malaria infection.
These are distinct goals: elimination is achievable on a country or regional level, while eradication requires global coordination and sustained effort across all endemic areas.
Globally, the elimination net is widening, with more countries moving towards the goal of zero cases of malaria each year.
Vector control
This is the main way to prevent and reduce malaria transmission. When malaria was more prevalent and widespread globally, many countries eliminated the disease by removing mosquito habitat and breeding sites. This was done by:
- Changing land use
- Draining swamplands containing stagnant water
- Regular, extensive fumigation of areas using insecticides such as DDT
Fumigation using DDT is still carried out in many tropical and sub-tropical countries and can be effective in reducing mosquito numbers.

Environmental consequences
Both of these methods have environmental consequences:
- Changing habitat impacts on other species
- The application of insecticides kills honey bees and other pollinators
- Affects human health
For example, it is thought that DDT can be ingested and passed through the food chain. WHO recommends the following methods of vector control:
Insecticide-treated mosquito bed nets (ITN)
Sleeping under an ITN is seen as a particularly effective low-cost strategy as it provides a physical barrier with an insecticide effect.

The insecticide woven into the net kills mosquitoes so they cannot go on to bite others who may not be protected. Bed nets can reduce transmission by as much as 90% in areas with high coverage.
In 2018, about half of all people at risk of malaria in Africa were protected by ITNs, though this proportion has not increased significantly in recent years.
Insecticide-treated nets work on two levels: they provide a physical barrier preventing mosquito bites during sleep (when most malaria transmission occurs), and the insecticide kills mosquitoes that come into contact with the net, providing community-level protection. Regular replacement and proper use are essential for maintaining effectiveness.
Indoor residual spraying (IRS)
Spraying indoor surfaces with pyrethroid insecticides can also reduce malaria transmission. To gain significant community protection, IRS should be implemented at a high level of coverage. However, usage has declined across most WHO regions. This is partly because there is evidence of Anopheles mosquitoes developing an increasing resistance to pyrethroid insecticides. Many countries are switching to more expensive alternatives to mitigate mosquito resistance to pyrethroids.
Insecticide resistance is an emerging threat to malaria control efforts. As mosquitoes develop resistance to commonly used chemicals, control programmes must adapt by using more expensive alternatives, rotating different insecticide classes, or combining multiple approaches. This increases costs and complexity of control programmes.
Mosquito coils
Mosquito coils are used in some parts of the world. They are burned to emit a repellent smoke that controls mosquito invasion, but studies have shown they are only between 24% and 64% effective. Their use has also been discouraged by WHO because they emit other pollutants such as:
- Sulphur dioxide
- Nitrogen dioxide
- Volatile organic compounds (VOCs)
Medical interventions
Anti-malarial drugs
Some medicines can be used to prevent malaria by suppressing the blood stage of the infection. WHO has recommended intermittent preventative treatment for:
- Pregnant women
- Infants living in moderate to high transmission areas
Additional seasonal doses of medicine in areas of sub-Saharan Africa are also recommended. Unfortunately, Plasmodium resistance to anti-malarial drugs, such as chloroquine, is a recurring problem.
Vaccines
Until the last few years, there were no vaccines available to prevent malaria. The first and only one to be developed shows that it can significantly reduce malaria in young African children. It is RTS,S/AS01 (RTS,S), sold under the trade name Mosquirix, which acts against Plasmodium falciparum. In large scale clinical trials, the vaccine prevented approximately four in ten cases of malaria over a four-year period.
The development of RTS,S represents a major breakthrough in malaria prevention, though its moderate efficacy means it must be used alongside other control measures rather than as a standalone solution. Research continues on developing more effective vaccines targeting different stages of the parasite's life cycle.
Treatment
Early diagnosis and treatment of malaria reduces disease, contributes to reducing transmission and prevents deaths. The most effective treatment for malaria sufferers is artemisinin-based combination therapy (ACT).
Global management strategies
To follow up the progress made by the Roll Back Malaria programme (part of the Millennium Development Goals), WHO has launched a global technical strategy for malaria from 2016-2030 as part of all the SDGs. The strategy sets ambitious but achievable global targets, including:
- Reducing both malaria case incidence and mortality rates by 90% by 2030
- Eliminating malaria in at least 35 countries by 2030
- Preventing a resurgence of malaria in all countries that are malaria free
The Global Malaria Programme
The programme co-ordinates WHO's global efforts to control and eliminate malaria. The programme is supported by an Advisory Committee (MPAC) that is made up of a panel of malaria experts.
High burden, high impact approach
In 2018, WHO called for an aggressive new approach to make faster progress in tackling malaria. The approach is being driven by 11 countries that carry a high burden of the disease, including:
- Burkina Faso
- Cameroon
- DRC
- Ghana
- India
- Mali
- Mozambique
- Niger
- Nigeria
- Uganda
- Tanzania
The approach builds on the principle that no one should die from a disease that can be diagnosed and prevented. Key elements include:
- Political will to reduce malaria burden
- Measures taken based on strategic information
- Better guidance and a co-ordinated national response
Key Points to Remember:
-
What is malaria? Malaria is a vector-borne disease transmitted by Anopheles mosquitoes carrying Plasmodium parasites, causing approximately 405,000 deaths annually with 67% being children under five
-
Geographic distribution: Sub-Saharan Africa bears 93% of malaria cases and 94% of deaths, with transmission strongly linked to environmental factors including temperature (16-32°C), altitude (<1,500m), rainfall and stagnant water
-
Socio-economic factors: Poor housing quality, high population density, low income and limited education significantly increase malaria risk, making it primarily a disease of poverty. Nearly two-thirds of the global burden is concentrated among the poorest 20% of the world's population
-
Health and economic impacts: The disease has severe health impacts including high fever, anaemia and potential death, plus major economic costs of US$15-18 billion annually and up to 40% of public health expenditure in affected regions
-
Control strategies: Key interventions include insecticide-treated bed nets (90% transmission reduction), indoor residual spraying, anti-malarial drugs and the new RTS,S vaccine, supported by WHO's 2016-2030 strategy aiming for 90% reduction in cases and elimination in 35 countries
-
Critical challenges: Insecticide resistance, drug resistance, and the complex relationship between poverty and malaria require integrated approaches combining disease control with broader socio-economic development