Economic and Social Development (AQA A-Level Geography): Revision Notes
Economic and social development
How development improves health
As nations progress through economic and social development, the conditions in which populations live typically improve significantly. This progress has a direct impact on health outcomes and the provision of healthcare services across society.
Economic developments that improve health
When economies grow and develop, several key changes occur that benefit population health:
Food production and supply become more reliable through technological advances. The Green Revolution, for example, introduced high-yielding crop varieties and modern farming techniques that dramatically increased food availability. This reduces malnutrition and famine-related diseases.
The Green Revolution's impact on health demonstrates how technological innovation in agriculture can have far-reaching consequences beyond just food production, directly affecting disease patterns and life expectancy across entire populations.
Transport infrastructure expands to enable better distribution of food supplies and medical resources. Improved roads, railways and ports mean that essential medicines and food can reach more remote areas, whilst also allowing patients to access healthcare facilities more easily.
Sanitation systems are installed, particularly in urban areas. Investment in drainage and sewage systems reduces exposure to human waste and contaminated water. This is crucial for preventing water-borne diseases like cholera and typhoid.
Trade networks develop, allowing countries to exchange manufactured goods and resources for a wider variety of foods and medicines. This diversification means populations are less vulnerable to local crop failures and have access to a broader range of medical treatments.
Social developments that improve health
Alongside economic progress, social changes contribute significantly to improved health outcomes:
Public health education raises awareness about hygiene practices and disease prevention. When people understand how diseases spread, they can take steps to protect themselves and their communities. This knowledge transfer is one of the most powerful tools for reducing infectious disease transmission.
Educational improvements mean more people can read and understand health information. Better education about sanitation and disease transmission helps break cycles of infection.
Medical technology advances such as antibiotics and vaccines have revolutionised disease treatment and prevention. The discovery of penicillin in 1928, for instance, transformed outcomes for many previously fatal infectious diseases.
Healthcare workforce development through better training programmes for doctors, nurses and midwives ensures more skilled professionals are available to treat patients effectively.
Aid and support programmes from international organisations like the UN and NGOs help build healthcare facilities and deliver medical services in areas that lack resources.
The connection to population growth
Socio-economic development typically triggers increased population growth rates. Initially, life expectancy rises and death rates fall, but fertility rates remain high due to established social norms and prior experience of high infant mortality. Parents continue having large families as a form of insurance, even though more children now survive.
Over time, healthcare improvements reduce infant mortality rates significantly. Combined with better access to contraception, this leads parents to choose smaller families. However, this fertility decline lags behind the mortality decline, creating a period of rapid population growth during the development process.
Epidemiological transition
Epidemiological transition is the process through which socio-economic development accounts for a change, over time, from infectious diseases to chronic and degenerative diseases becoming the primary causes of death in a population.
The concept was developed by Abdel Omran in 1971, who observed that as countries modernise from developing to developed status, the pattern of diseases affecting their populations undergoes a fundamental shift. This transition is closely linked to the demographic transition model and is explained by advances in medical technology, disease prevention methods and improved access to healthcare.
The five stages of epidemiological transition
Omran originally identified three distinct phases, which were later expanded. The model now recognises five potential stages:
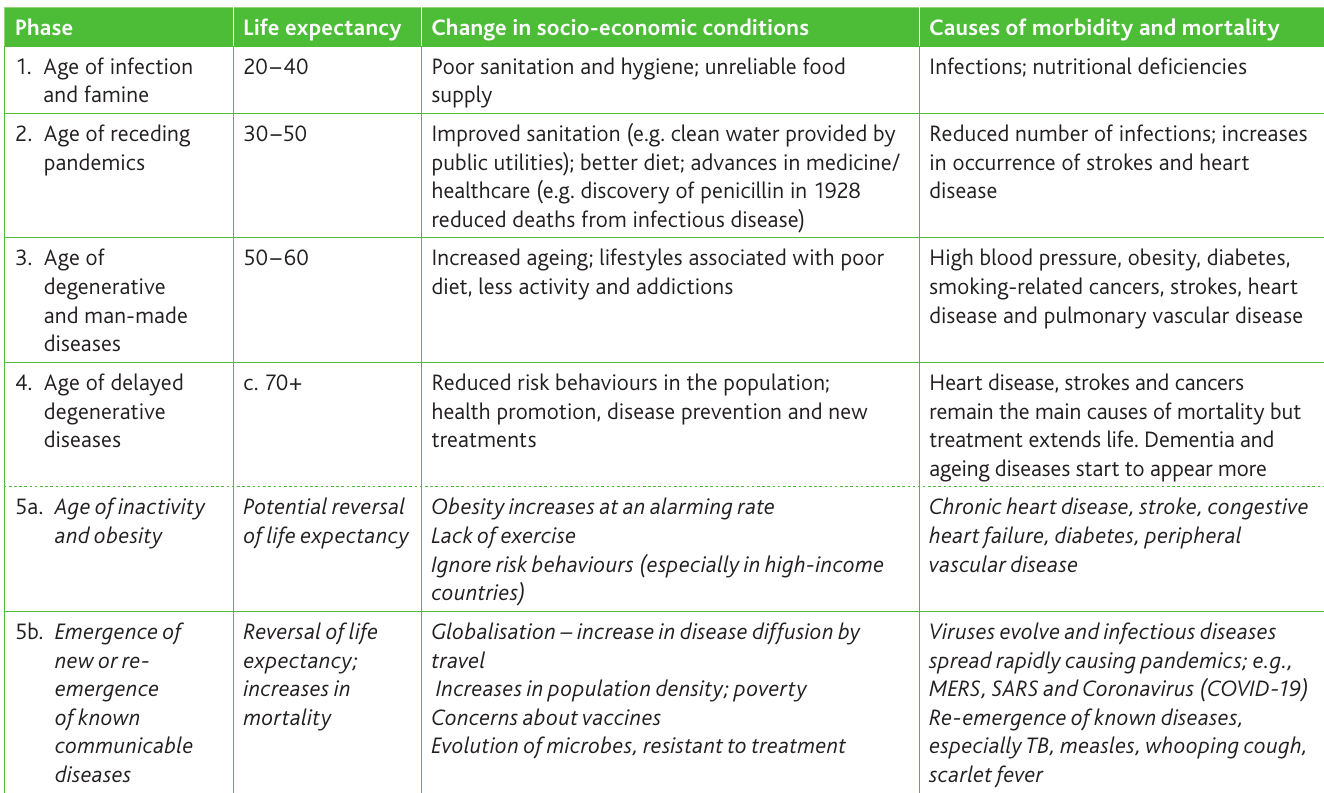
Stage 1: The age of infection and famine characterises pre-industrial societies where life expectancy ranges from just 20 to 40 years. Mortality fluctuates dramatically due to wars, famines and epidemic outbreaks, interrupted by brief periods of relative prosperity. Poor sanitation, unreliable food supplies and lack of medical knowledge mean infectious diseases and nutritional deficiencies dominate as causes of death. Population growth remains low and cyclical.
Stage 2: The age of receding pandemics sees mortality rates begin to decline as disease epidemics become less frequent. Life expectancy increases to 30-50 years. This stage is marked by improved sanitation (such as clean water supplied by public utilities), better healthcare provision, and advances in medicine like the discovery of penicillin in 1928. Whilst infections still occur, their frequency and severity reduce. Population growth becomes sustained and begins to increase exponentially.
The transition between Stage 1 and Stage 2 represents a critical turning point in human development history. The introduction of public health measures, particularly clean water and sewage systems, often had more impact on mortality rates than medical advances during this period.
Stage 3: The age of degenerative and man-made diseases represents a major turning point. Mortality continues declining and stabilises at relatively low levels, with life expectancy reaching 50-60 years. Infectious diseases are no longer the primary threat to life. Instead, chronic conditions caused by lifestyle factors become the main contributors to both morbidity (illness and disease in a population) and mortality. High blood pressure, obesity, diabetes, smoking-related cancers, strokes and heart disease now dominate. Fertility rates decline and become a more significant factor in determining population growth.
Stage 4: The age of delayed degenerative diseases emerges as death rates concentrate at advanced ages (70+ years). Risk behaviours reduce across the population as health promotion campaigns take effect and new treatments extend life. Heart disease, strokes and cancers remain the leading causes of death, but people live longer with these conditions. Dementia and other ageing-related diseases become more prevalent as life expectancy increases.
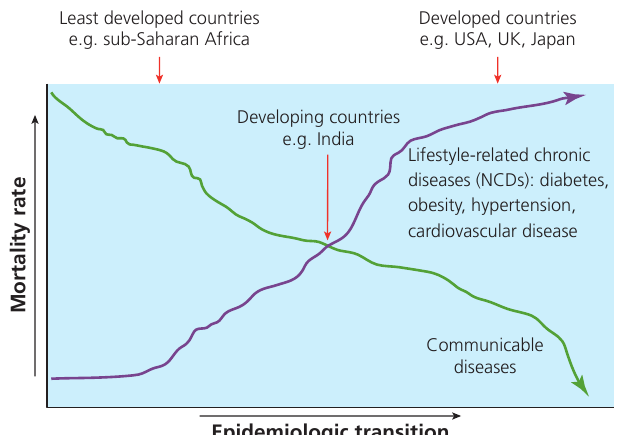
The model below illustrates how the balance between communicable and non-communicable diseases shifts as countries progress through development:
A possible fifth stage?
Since researchers added the fourth stage in the 1980s, debate has emerged about whether the world's population is entering a fifth stage of transition. Two main scenarios have been proposed:
Stage 5a: The age of inactivity and obesity suggests that life expectancy may begin to reverse in high-income countries. Obesity is increasing at an alarming rate, and sedentary lifestyles mean many people, particularly in wealthy nations, engage in insufficient physical activity. Poor dietary choices compound these risk behaviours. This could lead to chronic conditions like heart disease, stroke, congestive heart failure, diabetes and peripheral vascular disease causing earlier deaths and reversing previous gains in longevity.
Stage 5b: The emergence or re-emergence of communicable diseases focuses on the threat of infectious diseases spreading rapidly to cause pandemics. Globalisation has increased disease diffusion through international travel. Population density in urban areas facilitates transmission. Public concerns about vaccine safety have reduced immunisation rates in some areas. Additionally, microbes are evolving and developing resistance to treatments. Known diseases like tuberculosis (TB), measles, whooping cough and scarlet fever are re-emerging, whilst new viruses such as COVID-19, MERS and SARS have appeared as significant threats.
Some researchers have suggested a more optimistic scenario - an 'Age of Healthy Living' based on good diet and regular exercise. However, these ideas are not mutually exclusive, and it is likely that global populations will experience a mixture of all these trends in coming decades.
The pace of transition
Omran identified that whilst all countries undergo epidemiological transition, the pace and pattern vary significantly. He described three types of model:
Classical/western model (exemplified by Western Europe) features a slow decline in death rates followed by gradually declining fertility. The transition occurs over an extended period.
Accelerated model shows more rapid change, with mortality rates falling over a shorter timeframe. Many parts of Asia and some regions of Latin America have experienced this compressed transition.
Contemporary/delayed model describes situations where recent decreases in mortality are not matched by declining fertility rates. This occurs because infant and maternal mortality remain relatively high, as seen in sub-Saharan Africa. The demographic transition is delayed or incomplete.
Evidence supporting epidemiological transition
The theory of epidemiological transition asserts that infectious diseases like influenza, yellow fever, smallpox, malaria and tuberculosis are progressively replaced by chronic and degenerative conditions such as heart disease, cancer and dementia as the leading causes of death.
Historical data from the United States demonstrates this shift clearly:
Evidence from USA: The Epidemiological Transition in Action (1900-2010)
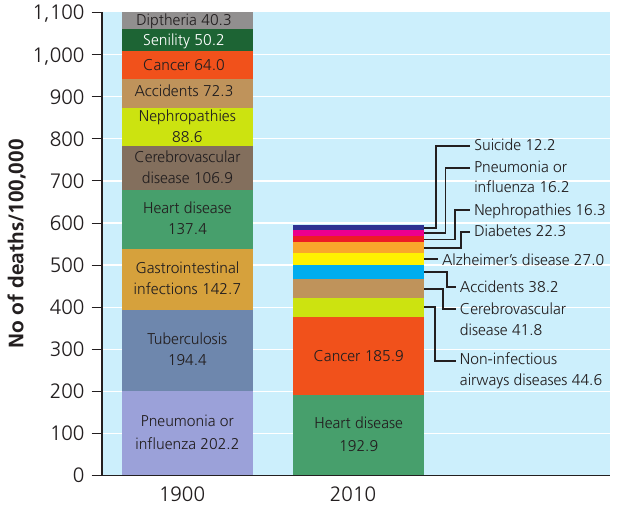
In 1900, the leading causes of death were predominantly infectious diseases:
- Pneumonia and influenza: 202.2 deaths per 100,000 population
- Tuberculosis: 194.4 deaths per 100,000
- Gastrointestinal infections: 142.7 deaths per 100,000
- Total mortality rate: approximately 1,100 deaths per 100,000 population
By 2010, the disease profile had transformed completely:
- Overall mortality rate: 600 deaths per 100,000 (a reduction of about 45%)
- Heart disease: 192.9 per 100,000 (now the leading cause)
- Cancer: 185.9 per 100,000
- New causes emerged: Alzheimer's disease (27.0 per 100,000) and diabetes (22.3 per 100,000)
Key transformation factors:
- Improvements in public health measures
- Better healthcare provision
- Vaccination programmes
- Development of antibiotics
- Enhanced public sanitation and hygiene practices
Critics argue that some of the apparent transition may be exaggerated - more chronic degenerative conditions may have existed in earlier periods but remained undiagnosed due to limited medical knowledge and diagnostic capabilities.
International comparisons further support the concept of epidemiological transition. The table below shows stark differences in disease patterns between low-income and high-income countries:
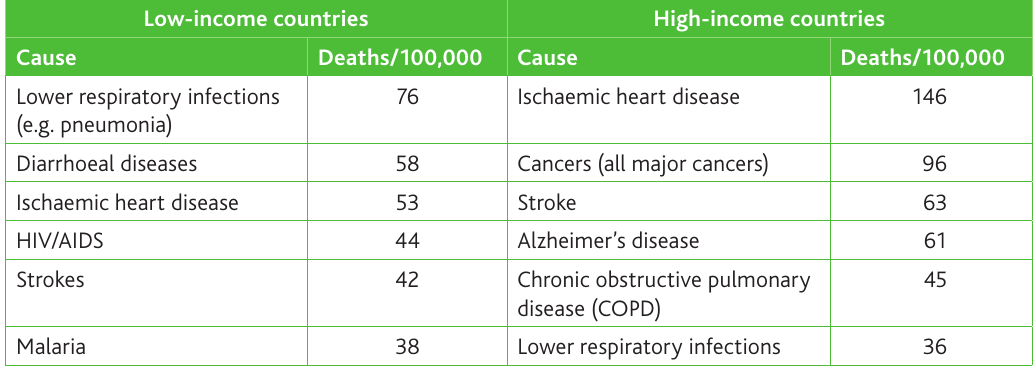
In low-income countries, infectious diseases dominate the mortality statistics. Lower respiratory infections like pneumonia cause 76 deaths per 100,000 population. Diarrhoeal diseases, HIV/AIDS, strokes, and malaria all feature in the top six causes of death. These are predominantly communicable diseases associated with poor sanitation, limited access to clean water, malnutrition, and inadequate healthcare infrastructure.
In contrast, high-income countries show a completely different pattern. Ischaemic heart disease leads at 146 deaths per 100,000, followed by all major cancers combined (96 per 100,000). Stroke, Alzheimer's disease, and chronic obstructive pulmonary disease (COPD) complete the top five. Lower respiratory infections still appear (at 36 per 100,000), but at much lower rates than in poorer nations.
According to World Health Organisation data, chronic degenerative diseases accounted for 46% of the global disease burden in 2001. By 2020, this proportion was expected to reach 57%. The proportion of degenerative disease is increasing rapidly in poorer countries, suggesting that epidemiological transition is advancing globally.
This means public health policy in developing nations faces a double burden - the traditional emphasis on controlling infectious disease must continue, whilst simultaneously adapting to address the growing challenge of chronic conditions.
Similarly, if global pandemics of infectious diseases like COVID-19 become more frequent, even high-income countries may need to adapt their healthcare systems and redirect resources to tackle periodic outbreaks whilst maintaining treatment for chronic conditions.
Environmental variables and disease
Climate and disease
The natural environment, particularly climatic conditions, plays a significant role in disease patterns. Drought conditions can lead to crop failures, reducing food consumption and potentially triggering famine. This weakens populations and increases susceptibility to disease.
At the opposite extreme, flooding caused by heavy rainfall or tropical storms can result in water-borne diseases and respiratory infections. When flood waters mix with sewage or contaminate water supplies, diseases like cholera, typhoid and dysentery can spread rapidly through affected populations.
Climate extremes demonstrate how environmental factors can quickly undermine public health infrastructure. Even developed countries with advanced healthcare systems can struggle when natural disasters compromise water treatment facilities or force population displacement into crowded emergency shelters.
Seasonal affective disorder
Seasonal affective disorder (SAD) is a type of depression that follows a seasonal pattern, with episodes of depression occurring at the same time each year.
SAD typically manifests during winter months and has been linked to reduced exposure to sunlight during shorter days. The lack of natural light appears to affect mood and energy levels in susceptible individuals. This condition demonstrates how environmental factors, even in developed countries with advanced healthcare systems, continue to influence health outcomes. The seasonal pattern is predictable, with symptoms typically worsening during the darkest months and improving as daylight hours increase in spring.
Remember!
Key Points to Remember:
-
Economic and social development drives health improvements through better food supply, transport infrastructure, sanitation systems, medical advances, education and healthcare access.
-
Epidemiological transition describes the shift from infectious to chronic diseases as countries develop. This occurs in stages from the 'age of infection and famine' through to the 'age of delayed degenerative diseases', with life expectancy rising from 20-40 years to 70+ years.
-
Evidence from the USA shows a 45% reduction in mortality rates between 1900 and 2010, with infectious diseases like pneumonia and tuberculosis being replaced by heart disease and cancer as leading causes of death.
-
Disease patterns differ dramatically between low-income and high-income countries. Low-income countries face predominantly infectious diseases (pneumonia, diarrhoeal diseases, HIV/AIDS), whilst high-income countries deal mainly with chronic conditions (heart disease, cancer, Alzheimer's disease).
-
A potential fifth stage is debated, with concerns about either reversing life expectancy due to obesity and inactivity, or facing re-emerging infectious diseases and new pandemics like COVID-19 threatening global health systems.