Sexual and Asexual Reproduction (HSC SSCE Biology): Revision Notes
Sexual Reproduction in Mammals
Introduction to sexual reproduction
Sexual reproduction in mammals involves the fusion of male and female gametes (sex cells) through a process called fertilisation. This creates a zygote (fertilised egg) containing genetic material from both parents. The genetic variation produced in offspring increases the population's chances of survival when environmental conditions change.
To make the energy investment of sexual reproduction worthwhile, mammals have evolved several mechanisms to maximise reproductive success:
- Internal fertilisation: This occurs in all three mammalian subclasses (monotremes, marsupials, and eutherians), increasing the likelihood that gametes will meet successfully.
- Implantation: In marsupials and eutherians, the embryo implants into the uterine wall where it develops internally, improving the embryo's survival chances.
- Pregnancy: The developing young are protected from external threats, receive a constant nutrient supply, and complete their development during gestation. Marsupials have short gestation periods, whilst eutherians have prolonged pregnancies, resulting in well-developed offspring at birth.
All stages of sexual reproduction are carefully controlled and synchronised by hormones that coordinate the reproductive cycle. Additional strategies that have evolved to increase offspring survival include timing of reproductive cycles, embryonic development within the uterus, reduced number of offspring produced, and quality parental care. Every stage from gametogenesis through courtship, pregnancy, and birth is hormonally regulated to ensure successful reproduction and species continuity.
Understanding hormones
Hormones are chemical messenger substances that coordinate many bodily functions, including metabolism and reproduction. They ensure that different actions within the body occur in a synchronised manner.
The Pituitary Gland: The Master Gland
The pituitary gland is a pea-sized endocrine gland located at the base of the brain, just above the roof of the mouth. Often called the "master gland", it secretes hormones that either stimulate or inhibit other endocrine glands throughout the body. This regulatory function controls the release of hormones involved in growth, metabolism, and reproduction.
Sex hormones are hormones that specifically affect the growth or function of reproductive organs, or the development of secondary sex characteristics. These hormones are produced in specialised tissues within the ovaries, testes, pituitary gland, and adrenal cortex. Although reproductive organs are present from birth in mammals, they only mature and become functional when stimulated by hormones secreted during puberty.
In humans, puberty typically occurs between ages and in girls, and ages to in boys. During this period, the gonads (reproductive organs) become functional and the reproductive cycle begins. Within the male and female gonads, gametes are produced through a process called gametogenesis.
Hormonal control of breeding seasons
Hormones regulate sexual behaviour in mammals by restricting reproduction in some species to specific times of the year, known as breeding seasons. In these seasonal breeders (such as sheep and cattle), breeding cycles involve periods where female fertility is limited to once or twice yearly. Mating only occurs during these fertile periods, when the animal is said to be 'on heat', 'in season', or biologically 'in oestrus'.
In contrast, higher-order primates (including humans) and some other mammals (such as pigs, rats, mice, and rabbits) are continuous breeders. In these species, female fertility occurs in cycles that repeat throughout the year, meaning they are sexually active year-round rather than having a restricted breeding season.
Advantages of Different Breeding Patterns
Both breeding patterns offer distinct advantages:
- Seasonal breeders typically give birth when temperatures are warm and food is abundant, increasing offspring survival rates. Parents also benefit from a limited period of mating, gestation, and raising young—a time when their energy reserves decline and vulnerability to predators increases.
- Continuous breeders have the clear advantage of their ability to reproduce throughout the entire year, providing more opportunities for successful reproduction.
Types of sex hormones
There are three main categories of sex hormones in mammals:
Androgens
Androgens (from the Greek andro meaning 'male') are commonly known as male hormones. They control the development and functioning of male sex organs and secondary sex characteristics including deepening of the voice, increased hair growth and thickness, and enlargement of muscles and bones. Cells in the testes secrete the androgen testosterone, which plays the primary role in spermatogenesis (sperm production).
Whilst androgens are present in both males and females, their production increases during puberty in both sexes. However, levels are significantly higher in males. Androgens also serve as precursor molecules for oestrogens.
Oestrogens
Oestrogens (from the Greek oistros meaning 'mad desire', referring to a female's willingness to mate during the fertile part of her cycle) form the main group of female hormones. They control the development and functioning of the female reproductive system and secondary sex characteristics such as breast enlargement, pubic hair development, and widening of the hips.
Although oestrogens are present in both sexes, they occur at much higher levels in females of reproductive age. In males, oestrogens work alongside testosterone to assist in sperm maturation. Oestrogens trigger the onset of oestrus (heat) just before ovulation in seasonal breeding mammals. The primary function of oestrogens in mammalian reproduction is controlling ovarian functioning and therefore female fertility.
Progestogens
Progestogens, the second group of female hormones, derive their name from pro (one) and the Latin gestare (to carry about, as in gestation). Progesterone is the most common progestogen and plays a crucial role in pregnancy. It also stimulates milk secretion in mammary glands (lactation), and a decrease in its levels helps initiate menstruation.
Modern Applications of Sex Hormones
Modern biotechnology allows artificial manufacture of female hormones for use either as contraception to prevent pregnancy or as fertility treatments to help women conceive. For example, progestin is the synthetically produced version of progesterone. Oestrogens and progesterone may be used in combination or individually for hormone replacement therapy during menopause or in treating prostate cancer and certain breast and endometrial cancers.
Hormonal control of the female reproductive cycle
Endocrine glands regulate and control the ovarian and menstrual cycles in a coordinated fashion, synchronising these cycles to ensure fertility. This coordination increases the probability of successful reproduction, biological fitness, and species continuity.
The pituitary gland secretes several hormones that regulate other endocrine glands, including the ovaries. Therefore, hormones from the pituitary and gonads are the key regulators of mammalian reproductive cycles.
Oestrogen and progesterone, produced by the ovaries and controlled by pituitary hormones, regulate:
- The ovarian cycle by controlling production and maturation of ova (eggs) in the ovaries
- The menstrual cycle by preparing the uterus for implantation of a fertilised egg each cycle; if fertilisation does not occur, oestrogen and progesterone levels decrease, causing the uterine lining to tear away accompanied by bleeding (menstruation)
- Maintenance of pregnancy
- Preparation for and maintenance of lactation
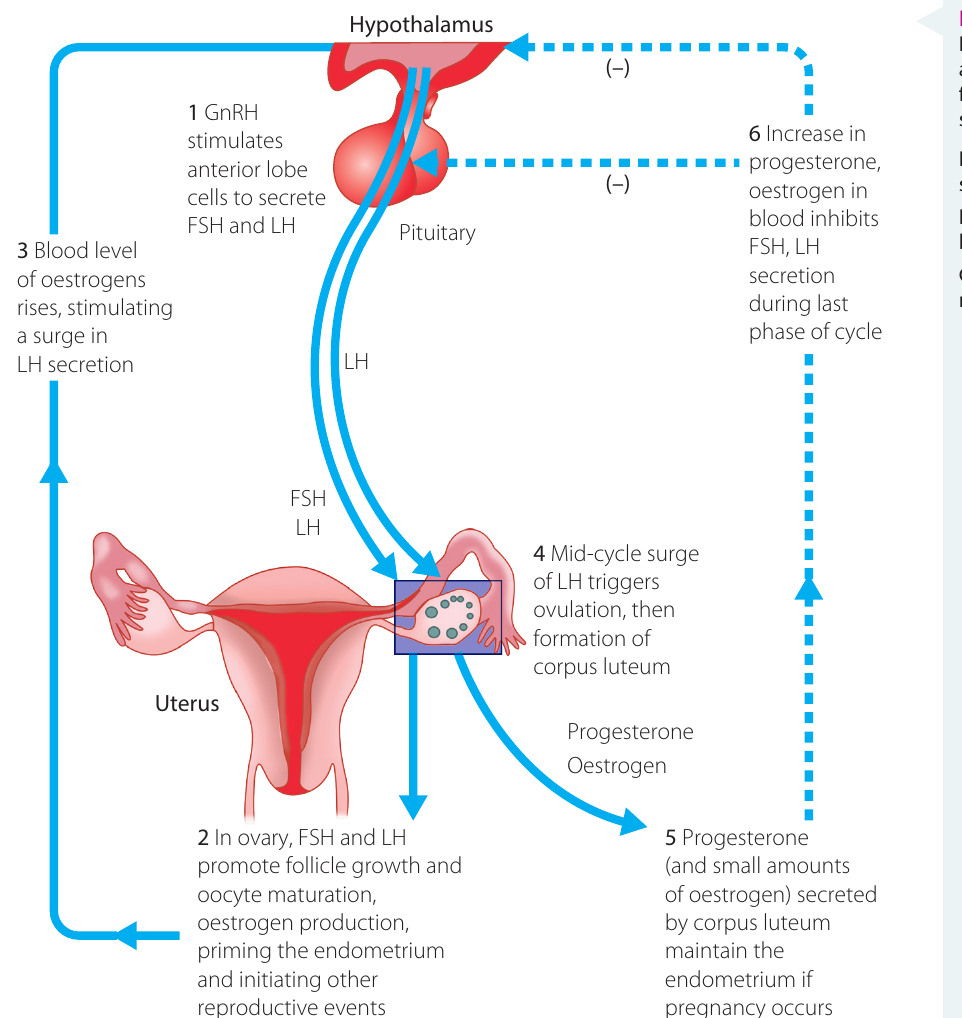
The pituitary secretes two gonadotropic hormones:
- Follicle stimulating hormone (FSH): Stimulates maturation of follicles in the ovaries
- Luteinising hormone (LH): Promotes final maturation of the ovarian follicle, triggers ovulation, and stimulates development of the corpus luteum. It also stimulates testosterone secretion
Additionally, the pituitary gland secretes prolactin, a lactogenic hormone that acts on breast tissue to prepare for and maintain milk production for suckling young.
The interaction between the pituitary gland and the ovaries and testes is synchronised through feedback loops, ensuring proper hormonal balance throughout the reproductive cycle.
The ovarian cycle
Female babies are born with all the eggs (ova) they will ever produce, though these ova are immature and only partly developed within their ovaries. During puberty, the ovarian and menstrual cycles begin—a process called menarche. The ova in the ovaries become surrounded by a single cell layer that divides, resulting in formation of primary (dormant) follicles.
Hormones secreted during puberty (and for approximately the following – years) trigger the development and maturation of ova each month, except during pregnancy. This continues until menopause is reached. At the start of each monthly cycle, several follicles begin developing, but typically only one enlarges beyond the others to reach full maturity. In humans, this cycle repeats approximately every days, though this timing varies between individuals.
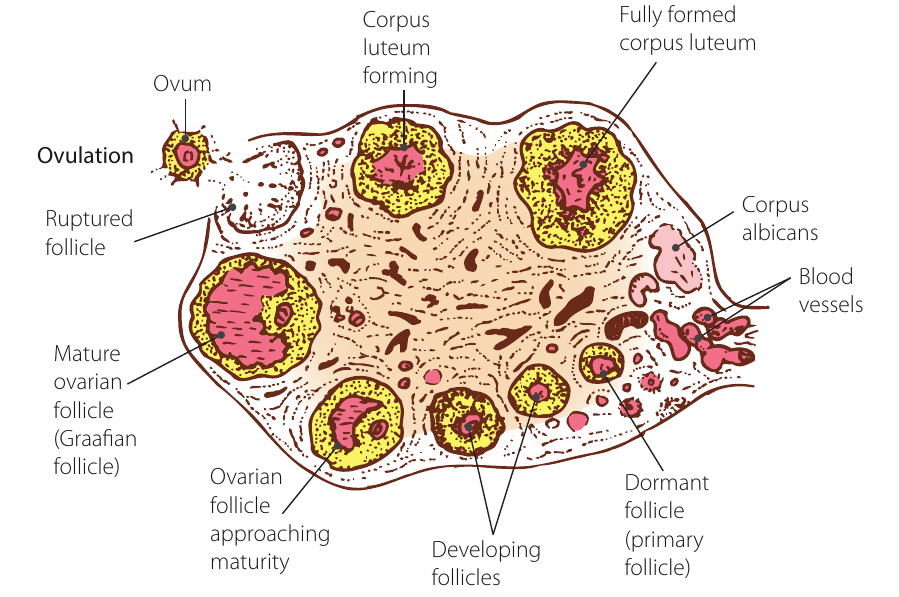
The follicle cells secrete fluid that pushes the egg to one side of the follicle. The enlarged, dominant follicle moves to the ovary's surface, creating a visible bulge. Once mature, it is termed a Graafian follicle. Development from primary follicle to Graafian follicle takes approximately – days.
During this follicular phase, cells lining the follicle secrete oestradiol (an oestrogen hormone). This triggers a surge in LH production, which results in ovulation. The LH surge also stimulates the next phase of the ovarian cycle, during which the corpus luteum forms and progesterone is synthesised.
The Graafian follicle bursts, releasing the egg in a process called ovulation. The funnel-shaped, open ends of the uterine tubes contain cilia that beat rhythmically, drawing the egg into the tube. The egg, with some follicle cells still attached, moves down the tube towards the uterus. If sperm are present, fertilisation may occur. Ovulation typically occurs mid-cycle.
Once released, the female ovum remains viable for only – hours. This narrow window of fertility makes precise timing crucial for successful fertilisation.
The luteinising phase
The luteinising phase usually lasts days. It begins after ovulation when the burst follicle in the ovary enlarges and changes colour as it accumulates a yellow protein called lutein. This large mass of vacuolated cells is now called the corpus luteum (Latin for 'yellow body'). The corpus luteum secretes progesterone, which acts on the uterus to prepare it for potential pregnancy.
The menstrual cycle
The ovarian cycle is accompanied by corresponding changes in the uterus, known as the menstrual cycle. An average menstrual cycle repeats every days, though considerable variation in actual cycle length is normal.
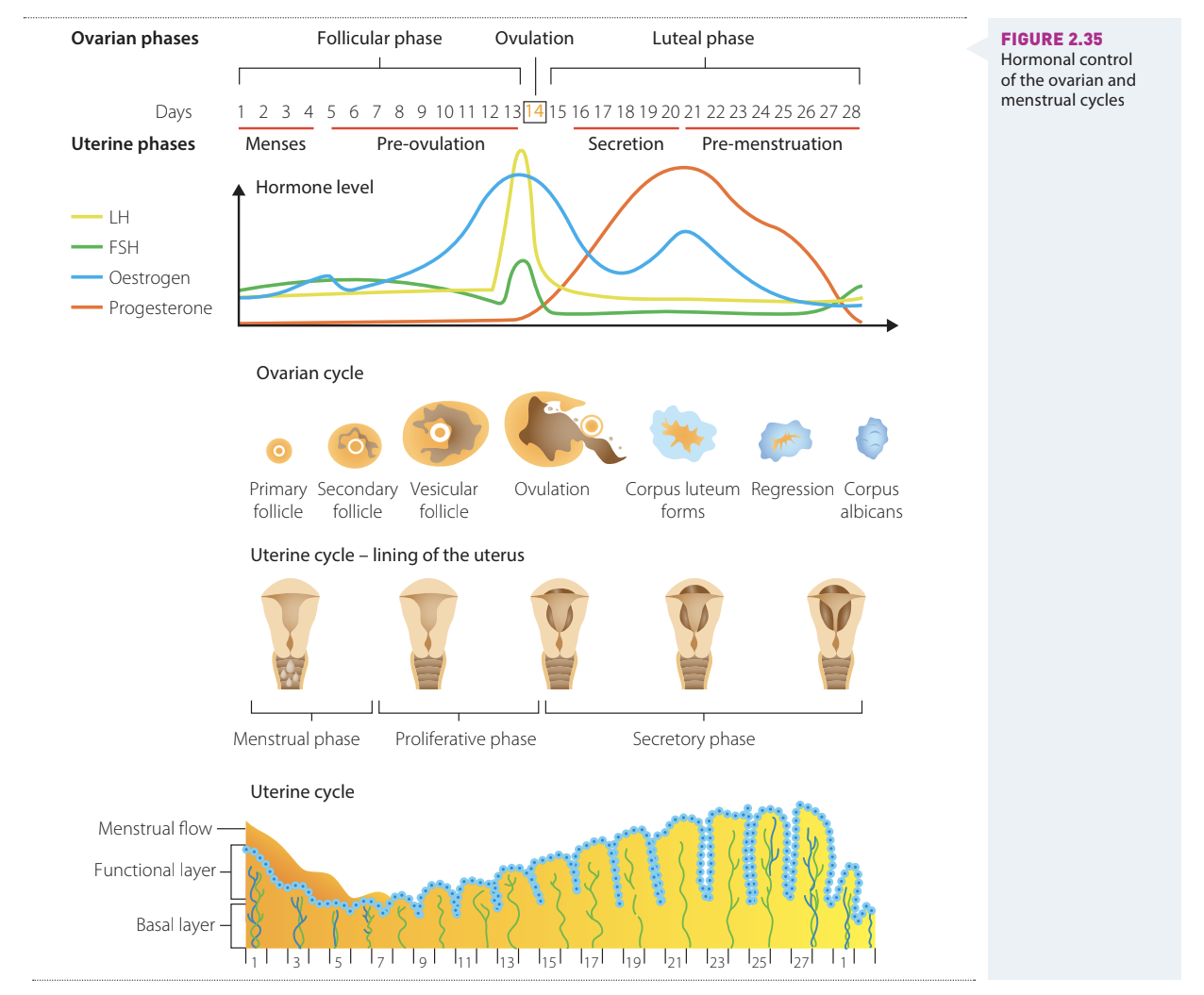
The menstrual cycle begins with menses (the menstrual period), lasting approximately four days. During this time, the endometrium (uterine lining) breaks down and tears away, accompanied by bleeding known as menstruation. The first day of menses marks the beginning of the follicular phase, which ends on ovulation day.
Following menstruation, a new endometrial lining forms in the uterus over approximately – days, called the pre-ovulation phase. Ovulation occurs in an ovary about – days after menstruation starts, though this timing varies between individuals.
After ovulation, the enlarging corpus luteum within the ovary secretes progesterone and some oestrogen into the bloodstream. Progesterone acts on target cells in the uterus, preparing the endometrium for implantation of a fertilised ovum and pregnancy. The endometrium becomes highly vascularised, reaching peak development or days after ovulation during the secretory phase, coinciding with the expected time of implantation. In this phase, endometrial glands secrete watery mucus.
If a fertilised ovum implants in the uterus, pregnancy begins and the uterine wall is maintained by progesterone and oestrogen secretion. Initially, the corpus luteum produces these hormones, but the placenta takes over this role later in pregnancy. During pregnancy, the placenta forms, attaching the developing embryo to the uterine wall. It secretes hormones including progesterone, oestrogen, and human chorionic gonadotropin (HCG) to maintain pregnancy. Once the placenta can produce these hormones, the corpus luteum begins to degenerate.
| Stage | Time span (days) | Events |
|---|---|---|
| Menstruation | – | Uterine bleeding accompanied by shedding of the endometrium |
| Pre-ovulation | – | Endometrial repair begins; ovarian follicle develops; uterine lining gradually thickens |
| Ovulation | – | Mature follicle ruptures, releasing egg |
| Secretion | – | Glands of endometrium, cervix, and uterine tubes secrete watery mucus; unfertilised egg moves and breaks down; corpus luteum develops |
| Pre-menstruation | – | Corpus luteum degenerates; endometrium deteriorates |
Note: Time spans are averages and vary widely between women.
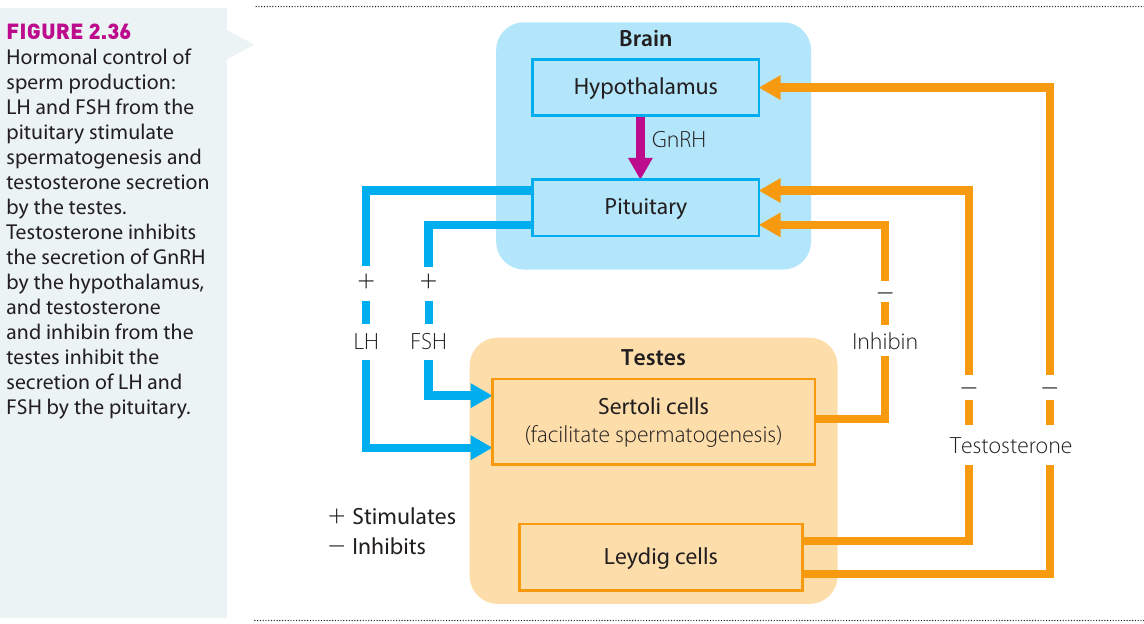
Hormonal control of the male reproductive cycle
Sperm production, or spermatogenesis, is controlled by hormones. In humans, spermatogenesis involves interaction between three glands: the hypothalamus in the brain, the pituitary gland at the brain's base, and the Leydig cells in the testes.
In males, LH stimulates testosterone production whilst FSH stimulates Sertoli cells in the testes to produce a protein that maintains testosterone at levels high enough to promote spermatogenesis. When the hormone inhibin is secreted, it reduces FSH levels in the body.
Sperm production in the male
Sperm are produced by meiosis inside sperm tubules in the testes and stored until mature. Each sperm is microscopic and tadpole-shaped, with an enlarged head containing the haploid nucleus and a long tail that whips side to side, enabling movement.
The Sperm's Journey
During copulation, semen containing sperm is introduced into the female's vagina. The sperm must undertake an challenging journey to reach the egg cell. Although around half a million sperm may begin this journey, only a few hundred to a few thousand reach the ovum. Vaginal wall contractions assist sperm movement. The whipping tail action is thought to keep sperm afloat in the semen and help penetrate the egg. Sperm can survive in the female reproductive tract for several days.
Fertilisation
Sperm are attracted to the egg through rheotaxis—movement through fluid—for internal fertilisation. Oviducts secrete fluid that travels down the female reproductive tract, and sperm swim upstream (positive rheotaxis). Sperm reaching the oviduct are stored and released in small batches. The presence of progesterone and an alkaline pH cause sperm to mature, enabling egg penetration. These mature sperm become hypermobile, with tails beating strongly to propel them toward the egg.
The Three Protective Layers
When sperm reach the egg cell, they must cross three protective layers:
- The first membrane, which still has follicle cells attached
- The zona pellucida (penetrated using enzymes from the acrosome)
- The cell membrane (plasma membrane), which only allows one sperm to penetrate
When sperm reach the egg cell, they must cross three protective layers. They physically push through the first membrane, which still has follicle cells attached. These protective cells release enzymes assisting sperm penetration. When a sperm's acrosome (protective cap) contacts glycoproteins of the next barrier (zona pellucida), the acrosome fuses with the sperm head's cell membrane, allowing the sperm tip to release enzymes that assist penetration.
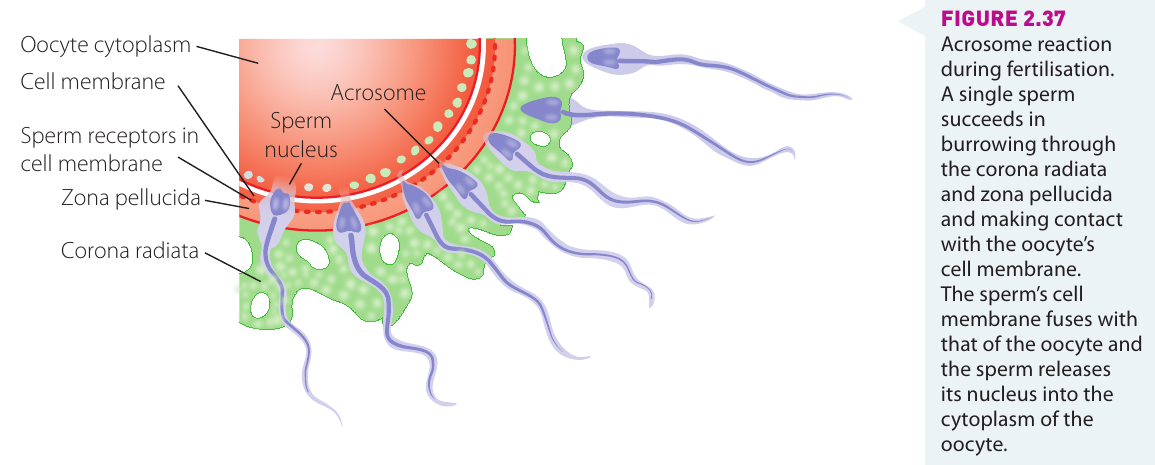
Many sperm may reach the final barrier, the cell membrane (plasma membrane). Surface proteins allow only one sperm to penetrate, triggering enzyme release by the egg that destroys glycoproteins in the zona pellucida and causes electrical changes, preventing other sperm entry. The first sperm to penetrate this inner barrier causes the ovum to immediately undergo its second meiotic division.
Fertilisation occurs when the haploid nucleus of the egg fuses with the sperm nucleus, forming a diploid fertilised egg called the zygote. At this stage, most epigenetic markers from the parents are removed from the DNA, switching all genes on—a process that remains an active area of research. Following fertilisation, the egg divides as it travels along the oviduct and begins developing into an embryo.
Hormonal control of pregnancy and birth
When the embryo implants into the uterine wall, pregnancy begins. Once implanted, the corpus luteum in the ovary continues growing and secreting hormones for the first three months of pregnancy. In the latter six months, the corpus luteum gradually shrinks and degenerates (though it remains present in degenerate form at childbirth). The placenta takes over hormone production to maintain pregnancy. Following pregnancy, the ovarian cycle typically only resumes once the mother stops breastfeeding.
If the egg is not fertilised, the corpus luteum begins degenerating approximately – days after ovulation, forming fibrous tissue called the corpus albicans. An unfertilised egg degenerates during pre-menstruation, after which menstruation occurs and the ovarian cycle begins again.
The environment in which the baby develops is rigorously controlled by hormones, important not only for growth and development to birth but also for long-term health. Hormones maintaining pregnancy are initially secreted by the mother's pituitary gland and ovaries, but once the placenta is established, it begins secreting hormones too.
The Critical Role of Hormones in Pregnancy
Oestrogen and progesterone levels are optimised during the ovulation cycle to create ideal conditions for implantation. Oestrogen promotes endometrial (uterine lining) growth whilst progesterone stimulates mucus secretion by endometrial lining cells and blood vessel growth. Once implantation occurs, progesterone's main role becomes suppressing uterine activity, thereby supporting foetal development and reducing the risk of the foetus being disturbed or expelled by uterine contractions. Progesterone also reduces the mother's immune response to foetal antigens. Adequate progesterone production by the corpus luteum is essential for maintaining pregnancy until the placenta assumes this function around – gestational weeks.
Other hormones are also important in maintaining pregnancy and ensuring normal baby development and growth. Some hormones prevent foetal overgrowth whilst others inhibit overgrowth at various pregnancy stages, mainly by regulating the amount and types of nutrients crossing the placenta.
| Hormone | Secreted by | Active period during pregnancy | Effect on pregnancy | Effect on foetal development |
|---|---|---|---|---|
| Maternal thyroxin | Mother's thyroid gland | From gestational weeks | Low levels increase risk of placental detachment and pregnancy loss | Low levels result in low birth weight and immature lungs |
| Insulin | Foetal pancreas (mother's insulin does not cross placenta) | From gestational weeks | No effect | Promotes foetal growth, allowing glucose availability for tissue growth and fat deposition |
| Human chorionic gonadotropin (hCG) | Developing embryo | First trimester of pregnancy (pregnancy tests measure this hormone) | Maintains corpus luteum, which helps maintain endometrium | No effect |
| Insulin-like growth factors (IGF) | Uterine wall of mother | No effect | IGF I: alters placental nutrient transport, matching to foetal demand; IGF II: stimulates placental growth | Promotes foetal tissue growth |
| Glucocorticoids (cortisol and cortisone) | Foetus | Increase during third trimester; elevated if mother becomes stressed or anxious | Maternal alcohol intake during pregnancy stimulates glucocorticoid secretion, leading to low birth weight and affecting organ development | Limits foetal growth; promotes and coordinates specialisation and development of foetal tissues and organs (e.g. brain, heart, lungs) |
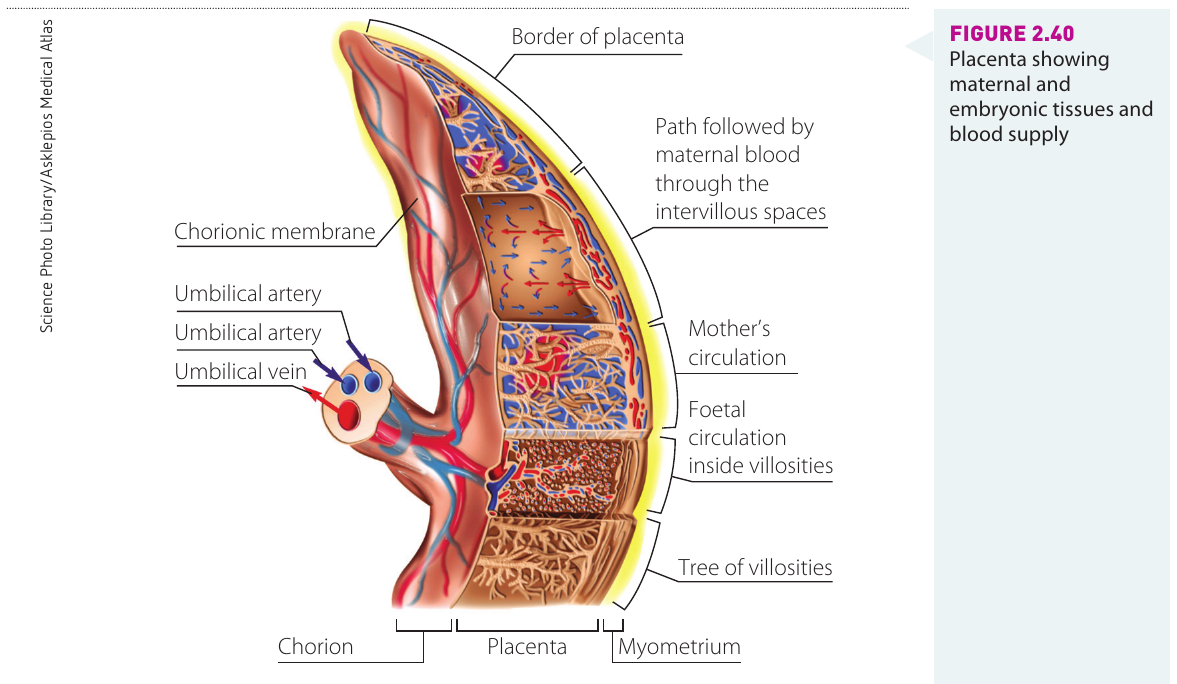
The Placenta: A Vital Exchange Interface
The placenta is a large disc of tissue formed from both maternal and foetal tissue. Each side produces finger-like extensions called villi—extensions from the mother's uterine wall form some villi, which interlace with extensions from the chorion membrane surrounding the foetus (chorionic villi). The placenta, embedded in the uterine wall, connects to the foetus via an umbilical cord carrying blood vessels to and from the baby. The placenta transports oxygen and nutrients from mother to foetus and removes wastes such as carbon dioxide and urea from the foetus, passing them to the mother for excretion. These gases, nutrients, and wastes diffuse across the narrow space between the villi. Crucially, the mother's and baby's blood do not come into direct contact.
Birth
Two essential processes must occur for birth:
- The uterine muscles must contract to expel the baby
- The cervical tissue must soften so the cervix can dilate (widen) to allow the baby's passage
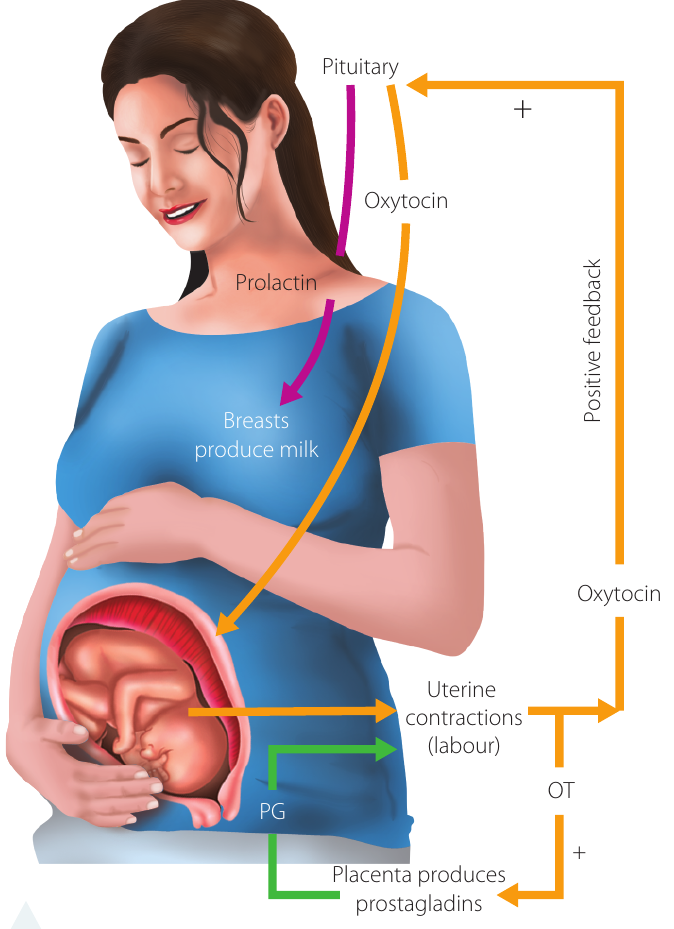
What triggers childbirth remains largely unknown. Prostaglandins secreted by the uterine wall initiate labour by making uterine tissue more sensitive to another hormone, oxytocin.
The Birth Process
Oxytocin promotes coordinated contraction of the uterine smooth muscle and softening (ripening) of the cervix, enabling birth. The hormone relaxin is also produced, further aiding cervical softening.
Progesterone and oestrogen levels decline during labour and contractions strengthen. As contractions intensify, beta-endorphin hormones are released, acting as natural pain relief and promoting feelings of elation. Very close to birth, an adrenaline surge from the mother's body causes very strong contractions leading to birth.
After the baby's birth, oxytocin secretion continues briefly, causing the uterus to contract and expel the placenta (sometimes called the 'afterbirth'). These contractions also limit blood flow to the uterus, reducing maternal bleeding risk.
Prolactin is a hormone produced mainly in the pituitary gland (but sometimes also in the uterus and breasts). It stimulates milk production in the breasts. Prolactin levels begin rising during the second trimester of pregnancy, causing mammary gland enlargement for milk production. Both prolactin and oxytocin release are further stimulated by the baby's suckling. These hormones are also thought to play important roles in maternal behaviour and bonding.
Key Points to Remember:
- Sexual reproduction in mammals involves fertilisation—the fusion of male and female gametes to form a zygote containing genetic material from both parents.
- Mammals maximise reproductive success through internal fertilisation, implantation of the embryo into the uterine wall, and pregnancy to protect and nourish the developing young.
- All stages of sexual reproduction are carefully timed and synchronised by hormones, including FSH, LH, oestrogen, progesterone, and testosterone.
- The ovarian cycle involves the follicular phase (follicle development and maturation) and luteinising phase (corpus luteum formation and progesterone secretion).
- The menstrual cycle prepares the uterus for potential pregnancy; if fertilisation does not occur, the endometrial lining breaks down during menstruation.
- Fertilisation occurs when sperm swim upstream through the female reproductive tract, penetrate the egg's protective layers, and fuse nuclei to form a diploid zygote.
- Pregnancy is maintained by hormones from the corpus luteum initially, then from the placenta, which also exchanges nutrients and wastes between mother and foetus.
- Birth is triggered by prostaglandins and oxytocin, which cause uterine contractions and cervical dilation, whilst prolactin stimulates milk production for the newborn.