Differences Between Male and Female Population Groups (VCE SSCE Health and Human Development): Revision Notes
Differences Between Male and Female Population Groups
Introduction
The health status of males in Australia has consistently been lower than that of females throughout history. While there have been some improvements in recent decades, males continue to experience shorter life expectancies and higher rates of many health conditions compared to females. Understanding these differences and the factors that contribute to them is essential for addressing health inequalities.
This topic examines the complex interplay of biological, sociocultural, and environmental factors that contribute to health disparities between male and female populations in Australia. Understanding these differences is crucial for developing targeted health interventions and policies.
Key differences in health status
Life expectancy and mortality
Males face higher mortality rates at every stage of life compared to females. A male baby born in 2019 can expect to live approximately four years less than a female baby born at the same time. This gap in life expectancy reflects the cumulative effect of various health disadvantages that males experience throughout their lives.
Males are more likely to die prematurely, with research showing that 62 per cent of all premature deaths occur in males. This means that males are much more likely than females to die before reaching their expected lifespan.
Critical Statistics on Male Mortality:
The four-year gap in life expectancy between males and females represents a significant public health concern. This difference is not simply a biological inevitability but results from a complex combination of modifiable risk factors that can be addressed through targeted interventions.
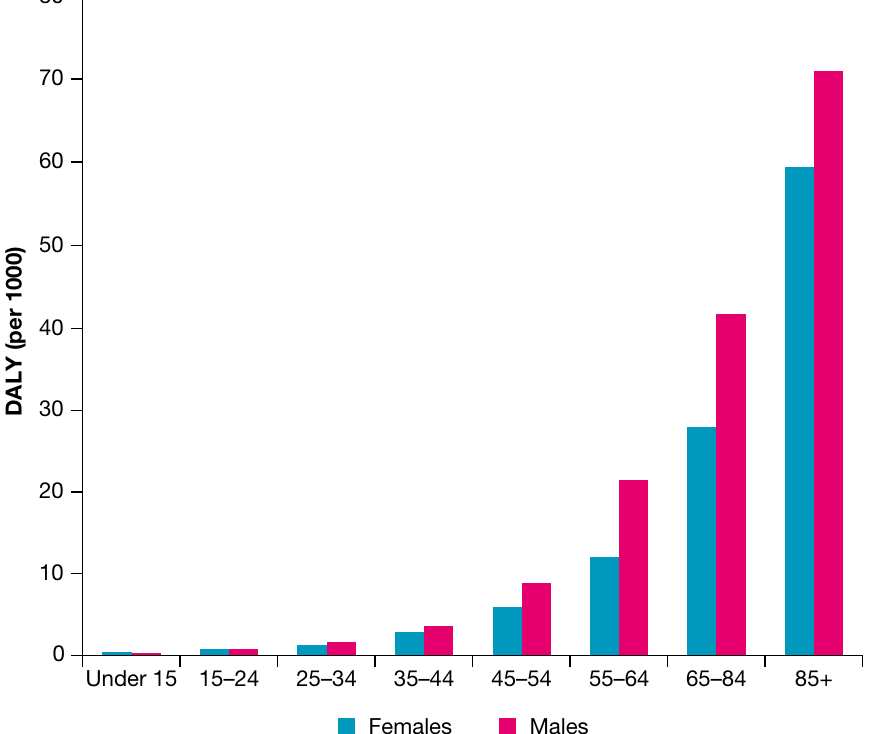
Burden of disease
Males experience a greater burden of disease than females across all age groups. This means they live with more years of ill health and disability throughout their lives. The difference in burden of disease becomes increasingly pronounced with age, particularly in older age groups.
Injury and accidents
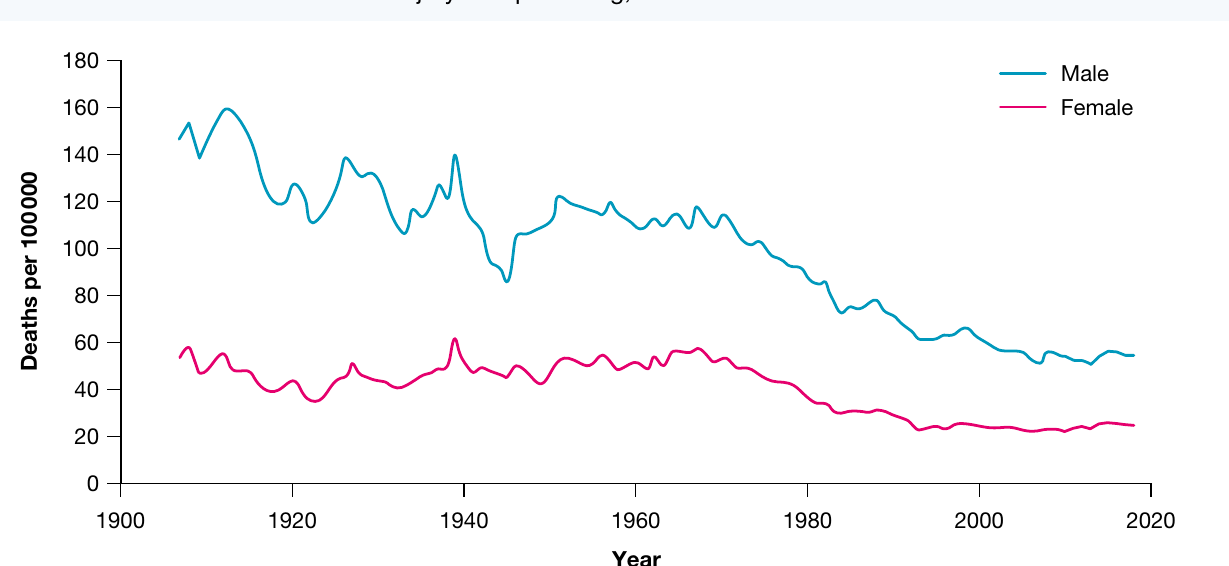
Males experience significantly higher rates of injury than females throughout the lifespan. The death rate from injury among males is approximately twice that of females. This difference reflects a combination of biological, sociocultural and environmental factors that increase male exposure to injury risks.

Males have substantially higher rates of deaths from specific causes of injury, including:
- Suicide
- Road trauma
- Violence
The graph below shows how injury-related death rates have changed over time for both males and females. While rates have declined for both groups, males consistently experience much higher rates.
Cancer
Males suffer higher rates of cancer overall. By age 75, one in three males will have been diagnosed with some form of cancer, compared to one in four females. More significantly, 56 per cent of all cancer deaths occur in males, indicating that males not only develop cancer more frequently but also experience worse outcomes.
Melanoma and Occupational Exposure:
Melanoma is particularly prevalent among males. By age 75, one in 23 males will have been diagnosed with melanoma, compared to one in 31 females. This difference is partly explained by greater occupational exposure to ultraviolet radiation among males, particularly those working in outdoor industries such as construction, farming, and landscaping.
Cardiovascular disease
Males are more likely to be diagnosed with cardiovascular disease and to experience heart attacks than females. The mortality rate from cardiovascular disease is also significantly higher for males, with 151.9 deaths per 100,000 males compared to 108.9 deaths per 100,000 females.
Diabetes and kidney disease
Diabetes affects 5.5 per cent of males compared to 4.3 per cent of females. Males also experience approximately 1.6 times higher mortality rates from diabetes than females. These higher rates of diabetes contribute to males experiencing higher rates of kidney disease, as diabetes is a major risk factor for kidney problems.
Respiratory disease
Males have higher mortality rates from chronic obstructive pulmonary disease (COPD) than females. This difference is associated with higher smoking rates among males historically, as well as occupational exposures to air pollutants and harmful substances.
Conditions where males fare better
Despite the many areas where males experience worse health outcomes, there are some conditions where males have an advantage:
Osteoporosis: Males experience much lower rates of osteoporosis than females. In fact, 85 per cent of all osteoporosis cases occur in females. This difference is primarily due to the protective effect of testosterone on bone density in males, compared to the loss of bone density that accelerates in females after menopause when oestrogen levels decline.
Arthritis: Males experience lower rates of arthritis, with 12.1 per cent of males affected compared to 17.9 per cent of females.
Mental health conditions: Males report slightly fewer cases of long-term mental and behavioural problems (17.9 per cent compared to 22.3 per cent of females). Males are also less likely to experience high or very high levels of psychological distress (11.3 per cent compared to 14.5 per cent of females).
Core activity limitations: Males are less likely to experience severe or profound core activity limitations. This means males are less likely to need help 'sometimes' or 'always' with core activities of daily living such as mobility, self-care or communication.
Factors contributing to variations in health status
Biological factors
Biological differences between males and females contribute significantly to variations in health status. These factors include body weight, blood pressure, glucose regulation and genetics.
Body weight
High body mass is more prevalent among males than females. Specifically, 42.0 per cent of males are classified as overweight compared to 29.6 per cent of females, and 32.5 per cent of males are obese compared to 30.2 per cent of females. When combined, these figures show that 74.5 per cent of males have a high body mass index compared to 59.8 per cent of females.
This higher prevalence of excess body weight among males contributes to increased rates of several conditions, including:
- Hypertension (high blood pressure)
- Cardiovascular disease
- Type 2 diabetes
The Impact of Body Weight on Male Health:
The significantly higher proportion of males with excess body weight (74.5% compared to 59.8% of females) represents one of the most modifiable risk factors contributing to health disparities. This single factor has cascading effects on multiple health conditions and is a key target for public health interventions.
Blood pressure
Males are more likely to experience hypertension than females throughout most of their lives. Until reaching the 65-74 age group, males have consistently higher rates of hypertension. After this age, females become more likely to experience high blood pressure.
Across all age groups below 65-74, approximately 25.4 per cent of males experience hypertension compared to 20.3 per cent of females. This difference contributes significantly to the higher rates of cardiovascular disease and kidney disease observed among males.

Glucose regulation
Males experience significantly higher rates of impaired glucose regulation than females. Impaired glucose regulation means the body has difficulty maintaining healthy blood sugar levels, which is a precursor to type 2 diabetes.
The higher rates of impaired glucose regulation among males contribute directly to their higher rates of type 2 diabetes and kidney disease. As males age, the burden of disease from impaired glucose regulation increases substantially, creating a compounding effect on overall health status.
Genetics
Several genetic differences between males and females contribute to health status variations:
Fat distribution: Males tend to store more fat around their abdomen compared to females. This pattern of fat distribution is associated with greater health risks, particularly for cardiovascular disease. This genetic tendency helps explain why cardiovascular disease is more common in males across almost all countries and cultures worldwide. Research continues to identify the exact genetic mechanisms responsible for this difference.
Hormones and bone density: Declining oestrogen levels at menopause accelerate bone density loss in women. In contrast, testosterone helps males maintain bone density throughout their lives. This hormonal difference explains the much higher rates of osteoporosis in females over age 60. Scientists are still investigating whether oestrogen provides protective effects against heart disease.
Testosterone and risk-taking: Higher levels of testosterone in males have been linked to increased risk-taking behaviours. This hormonal influence contributes to the higher levels of injuries that males experience compared to females, as males may be more likely to engage in dangerous activities or take unnecessary risks.
Sociocultural factors
A range of sociocultural factors influence health status differences between males and females. These include unemployment, socioeconomic status and cultural norms surrounding gender.
Unemployment
The effects of unemployment can be particularly severe for male health status. Traditionally, males have been viewed as the primary breadwinners for families, and many males feel a strong sense of duty to provide material resources for their household. When unable to fulfil this role through employment, males may experience feelings of inadequacy and stress that significantly affect their mental health and wellbeing.
Unemployment and Male Health Outcomes:
Research shows that unemployed males experience greater rates of morbidity and mortality compared to unemployed females. Specifically, unemployment is associated with higher rates among males of:
- Obesity
- Cardiovascular disease
- Suicide
This disparity highlights how deeply traditional gender roles can affect health outcomes when those roles cannot be fulfilled.
Socioeconomic status
Males employed on a full-time basis earn higher average incomes than females employed full-time. According to Australian Bureau of Statistics data from 2020, males earn an average of $1812.00 per week compared to $1558.40 per week for females. This income difference means males often have higher socioeconomic status than females, particularly compared to females who are single parents.
Higher socioeconomic status among males contributes to their lower rates of mental and behavioural problems and lower levels of psychological distress compared to females. This is because higher income provides better access to resources, healthcare, healthy food and safe housing.
Cultural norms and gender stereotypes
Gender stereotypes in Australia significantly influence health behaviours and outcomes for both males and females. These cultural expectations affect health in several ways:
Caring responsibilities: Males are less likely to be primary carers of children due to traditional gender roles. This means some males have more opportunities for social interaction with other adults than some females. Females who provide full-time care may experience social isolation, particularly if they don't have regular opportunities to communicate with people their own age. This isolation can negatively impact mental health and wellbeing, and may contribute to the higher rates of psychological distress experienced by females. Some females who lack adult social contact may 'bottle up' problems and issues rather than seeking support.
Physical labour: Physically demanding and laborious jobs are generally considered masculine occupations. This cultural expectation increases the risk of workplace injury for males who undertake such work, as these jobs often involve heavy lifting, operating machinery and other potentially dangerous activities.
Contact sports: Although female participation in sport has increased significantly, contact sports such as Australian Rules Football and Rugby League are still predominantly viewed as masculine activities. These sports carry inherent injury risks, and the cultural association with masculinity may encourage males to participate despite these risks, contributing to higher injury rates among males.
Healthcare Access and Masculinity:
According to the Australian Institute of Health and Welfare, males may be less likely to access healthcare than females. This reluctance is linked to social norms and values associated with traditional masculinity, including self-reliance, suppression of emotion and perseverance in the face of pain or discomfort. When males delay or avoid seeking medical care, health conditions may worsen before being diagnosed or treated, contributing to higher rates of morbidity and mortality.
Media representations: The media's portrayal of beauty differs significantly for males and females, with potential health consequences. Female beauty is often represented by thin models, while male beauty is typically portrayed through muscular figures. These different ideals have contributed to the higher prevalence of eating disorders among females. Media representations may influence eating and exercise patterns, particularly among young people trying to conform to these perceived ideals.
Peer pressure: The effects of peer pressure differ between males and females. When in groups, males may encourage traditional masculine stereotypes among their peers, including the use of violence to resolve conflicts, risk-taking behaviour and excessive alcohol consumption. These behaviours increase the incidence of injury, violence and alcohol-related harm among males.
Environmental factors
The work environment represents the primary environmental factor contributing to health status differences between males and females.

Occupational hazards
Males are more likely to work in industries with inherently dangerous environments, including:
- Trades (such as construction, plumbing, electrical work)
- Farming and agriculture
- Mining
These occupations involve several risk factors that can seriously affect health:
Heavy machinery and tools: Many male-dominated occupations require the use of heavy machinery and power tools, which increase the risk of serious injury or death from accidents.
Hazardous substances: Males working in trades, farming and mining face exposure to dangerous substances including chemicals, asbestos, pesticides and other toxic materials. This exposure increases the risk of respiratory conditions, cancer and other serious health problems.
Physical demands: These occupations often require significant physical exertion and can lead to musculoskeletal injuries, particularly affecting the back, shoulders and knees.
Workplace Fatality Statistics:
The concentration of males in dangerous occupations is starkly reflected in workplace fatality statistics. Of the 183 work-related deaths recorded in 2019, 177 (representing 97 per cent) involved male workers. The fatality rate for male workers was 30 times higher than the rate for female workers. This dramatic difference demonstrates how occupational choices and cultural expectations regarding appropriate work for males significantly impact mortality rates.
Outdoor work and UV exposure
Males are more likely to work outdoors in industries such as construction, farming, landscaping and mining. This outdoor work means males have increased exposure to ultraviolet radiation from the sun. The cumulative effect of this UV exposure helps explain the higher rates of melanoma and other skin cancers diagnosed in males compared to females. While sun protection measures can reduce this risk, males working outdoors may not consistently use adequate protection throughout their working lives.
Transport occupations
Males are more likely to work in transport-related occupations, including truck driving, delivery services and other roles requiring extensive time on public roads. This occupational pattern increases males' exposure to road trauma risks, as spending more time driving increases the probability of being involved in a serious accident. This contributes to the higher rates of injury and death from road trauma among males.
Summary of factors
The diagram below illustrates how biological, sociocultural and environmental factors interact to influence male health status:
How Factors Interact to Impact Male Health:
Consider a male working in the construction industry. This scenario demonstrates how multiple factors combine:
Biological factors: He may have a genetic predisposition to store abdominal fat and higher testosterone levels that influence risk-taking behaviour.
Sociocultural factors: Cultural expectations about masculinity may discourage him from seeking medical care when injured or unwell. He may also face peer pressure to engage in risky activities or excessive alcohol consumption after work.
Environmental factors: His occupation exposes him to heavy machinery, hazardous materials, and UV radiation. He spends significant time driving to job sites, increasing road trauma risk.
These factors compound to create significantly elevated health risks compared to the general population.
Remember!
Key Points to Remember:
-
Life expectancy gap: Males born in 2019 can expect to live approximately four years less than females, reflecting higher mortality rates at every life stage.
-
Three factor categories: Biological factors (body weight, blood pressure, glucose regulation, genetics), sociocultural factors (unemployment, socioeconomic status, gender stereotypes) and environmental factors (workplace hazards) all contribute to health differences between males and females.
-
Higher male risks: Males experience significantly higher rates of injury (death rate approximately double that of females), cardiovascular disease, diabetes, cancer and COPD, with 62% of premature deaths occurring in males.
-
Areas where males fare better: Males have lower rates of osteoporosis (85% of cases occur in females), arthritis, mental health problems and psychological distress compared to females.
-
Workplace impact: Males face substantially higher occupational risks, with 97% of work-related deaths in 2019 involving male workers, and male workplace fatality rates 30 times higher than female rates due to concentration in dangerous industries like mining, construction and farming.