Contributing Factors to the Development of Specific Phobia (VCE SSCE Psychology): Revision Notes
Contributing Factors to the Development of Specific Phobia
Understanding specific phobia
What is a specific phobia?
A specific phobia is a persistent, intense, irrational fear of a specific object or event. People with specific phobias experience fear that is disproportionate to any actual danger posed by the stimulus. This distinguishes phobias from ordinary fear, which serves a protective function.
Key characteristics of specific phobia include:
- Awareness that the fear is excessive or unreasonable
- Strong compulsion to avoid the phobic stimulus
- Fear response that is out of proportion to actual danger
- Organisation of daily life around avoiding the phobic stimulus
For a diagnosis of specific phobia, symptoms must:
- Persist for six months or longer
- Disrupt the person's life, particularly work and social relationships
- Cause serious distress
Categories of specific phobia
Phobias can be classified into four main categories:
- Natural environment phobias - fear of elements such as water, storms, or heights
- Animal phobias - fear of creatures such as snakes, spiders, or dogs
- Bodily pain or injury phobias - fear of needles, dental procedures, medical procedures, or the sight of blood
- Situational phobias - fear of confined or open spaces, aeroplanes, tunnels, or elevators

Specific phobia within the broader context of anxiety disorders
Specific phobia is one of several anxiety disorders. The table below outlines different types of anxiety disorders to provide context:
Anxiety is the most common mental health condition in Australia, affecting one in four people at some stage in their life. More than two million Australians experience anxiety each year. All anxiety disorders are characterised by worry, fear and anxiety that are strong enough to interfere with daily activities.
The biopsychosocial model and specific phobia
The biopsychosocial model provides a framework for understanding how mental and physical illnesses develop. This model recognises that biological, psychological, and social factors interact to influence health outcomes. Rather than viewing illness through a purely physiological lens, the biopsychosocial approach considers the whole person and their unique circumstances.
When understanding specific phobia, each of these three factors must be examined:
Even when two people receive the same diagnosis, the way these factors interact may differ significantly. Each person's case is considered individually, with all contributing factors identified to understand the extent of the illness and develop an appropriate treatment plan.
Biological factors
Biological factors relate to the physiological functioning of the body. These internal, physiologically based influences can contribute to the development, progression, or maintenance of specific phobia. Two key biological factors are GABA dysfunction and long-term potentiation.
GABA dysfunction
Gamma-aminobutyric acid (GABA) and glutamate are primary neurotransmitters that regulate arousal levels in the central nervous system. GABA functions as the main inhibitory neurotransmitter, blocking or reducing neural signals and decreasing nervous system activity. When GABA activates its receptors, post-synaptic neurons become less likely to fire action potentials, producing a calming effect that reduces anxiety, stress, and fear.
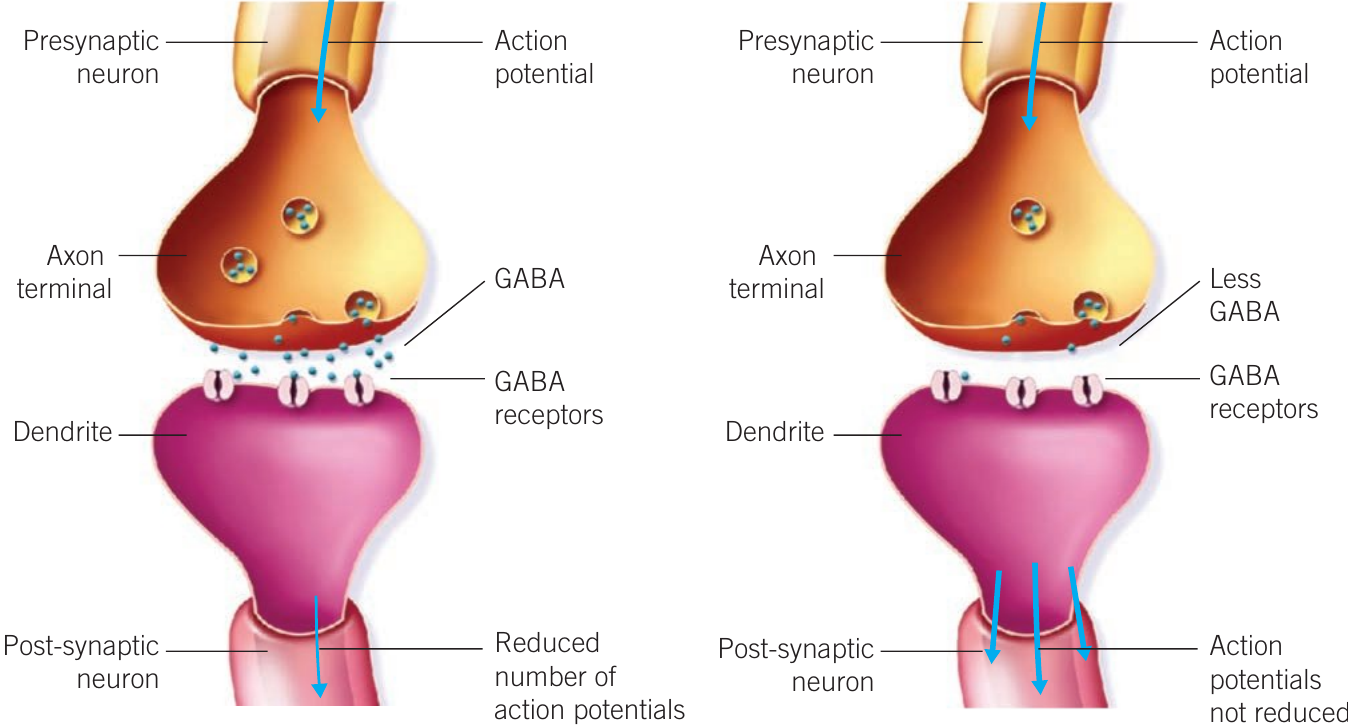
Research indicates that people diagnosed with specific phobia may have a dysfunctional GABA system - a failure to produce, release, or receive adequate GABA signals. This dysfunction creates a predisposition to anxiety.
When the GABA signal is insufficient, the inhibitory effect on neural activation is inadequate. This means the heightened arousal caused by excitatory neurons (releasing glutamate) during the fight-or-flight-or-freeze response cannot be properly regulated. Consequently, people with GABA dysfunction experience exaggerated feelings of fear or anxiety.
The impact of GABA dysfunction on phobia development can be understood through this pathway:
Individuals with low GABA signals are more vulnerable to anxiety. Their fight-or-flight-or-freeze response may activate more easily when they encounter or anticipate encountering a phobic stimulus, even when no real danger exists. This stress response can be severe and prolonged, maintaining anxiety feelings towards the fear object despite the imagined rather than real nature of the threat.
Long-term potentiation
Long-term potentiation (LTP) refers to the relatively permanent strengthening of synaptic connections as a result of repeated activation of a neural pathway. This neurobiological process enhances signalling between neurons and plays a role in learning and memory.
In the context of specific phobia, LTP strengthens the association between a phobic stimulus and fear or anxiety response. Each time the neural pathway connecting the phobic stimulus to the fear response is activated - whether through actual encounters with the stimulus or thinking about past or future encounters - the connection becomes stronger.

Example: LTP in Dog Phobia
Someone who was attacked by a dog repeatedly activates the same neural pathway between the memory of the dog attack and their fear of dogs whenever they think about the incident or encounter a dog. Through LTP, this neural pathway strengthens over time, intensifying the fear response and making the learned association much less likely to be forgotten.
Whilst fear can aid survival by helping us learn to avoid danger, LTP can contribute to maladaptive behavioural responses when the fear becomes a phobia. The strengthened neural pathways make the phobic response more automatic and harder to overcome.
Psychological factors
Psychological factors relate to the functioning of the brain and mind, including cognitive and affective processes such as thought patterns and memory. These internal influences associated with mental processes play a key role in both developing and maintaining specific phobia.
Behavioural models of phobia development
Behaviourism proposes that all behaviours are acquired through interaction with the environment. The behavioural model suggests that phobias are learned through experience and may be developed, sustained, or modified by environmental consequences such as rewards or punishments.
According to behavioural explanations:
- Classical conditioning precipitates (initiates or triggers) specific phobia
- Operant conditioning perpetuates (maintains or prolongs) specific phobia
Precipitation by classical conditioning
Classical conditioning is a learning process where a neutral stimulus becomes associated with an unconditioned stimulus through repeated pairing, eventually producing a conditioned response.
In phobia development, classical conditioning works through three stages:
Before conditioning:
- A neutral stimulus (e.g., a magpie) produces no particular response
- An unconditioned stimulus (e.g., being swooped) naturally produces an unconditioned response (e.g., shock and fear)
During conditioning:
- The neutral stimulus is repeatedly presented immediately before the unconditioned stimulus
- Each pairing of the neutral stimulus with the unconditioned stimulus produces the unconditioned response
After conditioning:
- The neutral stimulus has become a conditioned stimulus
- The conditioned stimulus alone now produces a conditioned response (fear)
Through this process, a previously neutral object or situation becomes associated with an intense fear response. The phobia has been precipitated through classical conditioning.
Stimulus generalisation may also occur, where the fear response extends to similar stimuli. For instance, someone who develops a fear of magpies through this process might generalise their fear to all birds.
Perpetuation by operant conditioning
Operant conditioning is a learning process where the likelihood of a voluntary behaviour occurring is determined by its consequences. In specific phobia, operant conditioning maintains the phobia through negative reinforcement.
Negative reinforcement occurs when a behaviour is followed by the removal of an undesirable stimulus, increasing the likelihood of that behaviour occurring again.
In the context of phobia:
When someone with a phobia encounters or anticipates encountering the phobic stimulus, they experience unpleasant feelings of fear or anxiety. By using avoidance behaviour - actions taken to escape from these difficult thoughts and feelings - they reduce or remove these unpleasant sensations. This reduction in anxiety negatively reinforces the avoidance behaviour, making the person more likely to avoid the phobic stimulus in future.
This creates a self-perpetuating cycle: avoidance provides temporary relief but prevents the person from learning that the feared stimulus may not be as dangerous as believed, thereby maintaining the phobia.
Cognitive biases
In contrast to the behavioural model, the cognitive model describes how people's perceptions of situations influence their emotional and behavioural reactions. When distressed, perceptions are often distorted.
The cognitive model examines distorted thinking patterns in the development and maintenance of specific phobia, focusing on how people process information about the phobic stimulus and related events. A key assumption is that people with specific phobia often demonstrate one or more cognitive biases - tendencies to think in ways that involve errors of judgement and faulty decision-making.
Memory bias
Memory bias is distorted thinking that either enhances or impairs the recall of a memory or alters its content. In people with specific phobia, memory bias operates in two main ways:
- Exaggeration of negative experiences: The person reconstructs memories to describe the phobic stimulus as bigger, more dangerous, or more frightening than it actually was. For example, someone with a moth phobia might remember an encounter with a moth as far more threatening than it truly was.
- Minimisation of positive or neutral experiences: The person forgets or downplays experiences that contradict their fear. For instance, someone with a kangaroo phobia might vividly remember the one time they were chased by a kangaroo but forget all the peaceful interactions they had with kangaroos.
This cognitive bias maintains the phobia by reinforcing a distorted, fear-focused view of the phobic stimulus whilst filtering out information that might challenge or reduce the fear.
Catastrophic thinking
Catastrophic thinking is a cognitive bias involving overestimating and exaggerating the worst possible outcomes to situations even though they are unlikely to occur.

People with specific phobia tend to predict the worst outcomes when thinking about encounters with their phobic stimulus, despite these predictions being unrealistic and irrational. Examples include:
- Someone with a dog phobia believing any dog will attack them and cause permanent injury
- Someone with a fear of driving believing they will certainly be injured or die every time they get in a car
When catastrophic thinking occurs, the person typically experiences heightened anxiety and distress whilst underestimating their ability to cope with the situation or their anxiety symptoms. This perpetuates the fear of the object or situation, as the exaggerated danger maintains avoidance behaviour and prevents the person from testing the reality of their fears.
Social factors
Social factors are external factors relating to the social components of a person's environment. These include skills in interacting with others and the range and quality of interpersonal relationships. Social factors represent the 'nurture' side of the nature versus nurture debate in understanding mental illness development.
Specific environmental triggers
A specific environmental trigger is an object, situation, or circumstance that causes a direct, negative, traumatic experience associated with extreme fear or discomfort, which then acts as a cue for future phobic fear responses.
Many people diagnosed with specific phobia report having had a negative and traumatic experience with the object of their phobia. They often attribute this specific encounter as the cause of their condition.

Examples of Specific Environmental Triggers
- A child experiencing sudden, extreme pain during an injection develops a phobia of needles
- Someone who nearly drowns develops a phobia of water
- A child attacked by a dog develops a fear of all dogs
The more traumatic the event - whether directly experienced or observed - the more likely a phobia will develop, even from a single occurrence. For instance, witnessing a terrible traffic accident where someone is covered in blood might later result in blood phobia.
However, specific environmental triggers do not explain all phobias. Not everyone exposed to similar traumatic events develops a phobia, as individual experiences and circumstances vary. Several factors influence whether a traumatic experience leads to phobia:
- Subsequent positive experiences: If a positive experience follows soon after the traumatic one, phobia is less likely to develop. For example, a child given a reward immediately after a painful injection, or someone who returns to water immediately after nearly drowning and has a positive experience, may not develop a phobia.
- Individual vulnerability: Biological factors (such as GABA dysfunction) and psychological factors may make some people more susceptible to developing phobias following traumatic experiences.

Stigma around seeking treatment
Stigma refers to negative stereotypes and feelings of shame or disgrace associated with a personal characteristic that indicates belonging to a culturally devalued group in society. This can be real or imagined.
People with specific phobia are particularly vulnerable to stigmatisation because:
- Phobias involve irrational fears that others may find difficult to understand
- Many phobic stimuli (such as balloons or buttons) are typically perceived as harmless
- People with phobias may be subject to ridicule, belittling comments, or disbelief
Three-quarters of people with mental illness report experiencing stigma. Research shows concerning attitudes towards mental illness in Australia, including beliefs that depression indicates personal weakness, that people with mental illness are unpredictable or dangerous, and reluctance to employ or vote for people with mental health conditions.
Stigma affects specific phobia in several ways:
Emotional impact: Stigma brings feelings of shame, poor self-esteem, and hopelessness, particularly when it results from a mental health disorder.
Worsening of symptoms: Distress and symptoms may intensify due to lack of understanding from family, friends, and others.
Barrier to treatment: Stigma prevents people from seeking help, as they fear judgement or discrimination. This perpetuates the phobia by allowing it to continue untreated.
By creating an environment where people feel unable to seek help, stigma plays a role in maintaining specific phobia and preventing recovery.
Remember!
Key Points to Remember:
-
Specific phobia is a persistent, intense, irrational fear of a specific object or event that leads to avoidance behaviour and disrupts daily life.
-
The biopsychosocial model explains that specific phobia develops through a complex interaction of biological, psychological, and social factors, with each person's experience being unique.
-
Biological factors include GABA dysfunction (which reduces inhibition of the fight-or-flight-or-freeze response, increasing vulnerability to anxiety) and long-term potentiation (which strengthens neural pathways linking the phobic stimulus to fear responses).
-
Psychological factors include behavioural processes (classical conditioning precipitates phobia by creating fear associations, whilst operant conditioning perpetuates phobia through negative reinforcement of avoidance) and cognitive biases (memory bias and catastrophic thinking maintain distorted, fear-focused perceptions).
-
Social factors include specific environmental triggers (traumatic experiences with an object or situation can initiate phobia) and stigma (negative stereotypes and shame prevent treatment-seeking, allowing the phobia to persist).