Animal Responses (HSC SSCE Biology): Revision Notes
Animal Responses
Introduction
Animals face constant exposure to a vast array of micro-organisms that could potentially cause disease. Complex multicellular organisms have evolved a multilayered system of defences to prevent infection and colonisation by pathogens. The animal immune system is highly organised, similar to an army, with different levels of defence and the ability to anticipate invasion by pathogens it has not yet encountered.
Lines of defence
The body's immune system consists of three organised levels of defence, each with specific roles in protecting against pathogens.
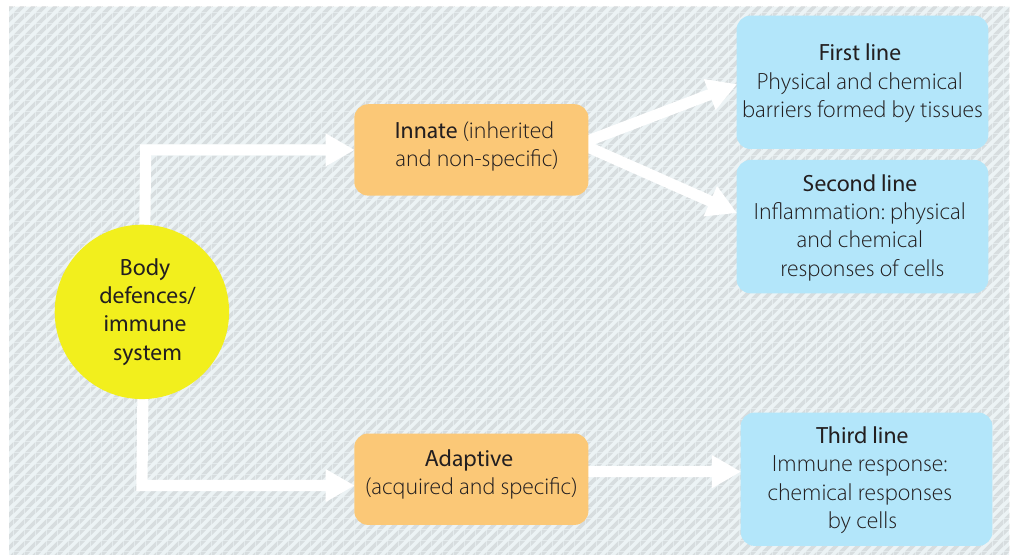
Think of the immune system as a multi-tiered security system: the first line prevents entry, the second line responds immediately if breached, and the third line provides targeted, specific responses to persistent threats.
Innate immunity
Innate immunity is present at birth and genetically determined. It provides non-specific responses to pathogens and includes:
- First line of defence: Physical and chemical barriers to pathogen entry
- Second line of defence: Cellular responses including inflammation and phagocytosis
These defences act against any substance recognised as 'non-self' and threatening, whether living organisms or non-living materials such as splinters, dust, or transplanted organs.
Adaptive immunity
Adaptive immunity is the third line of defence. This is a specific defence mechanism consisting of specialised cells (lymphocytes) that activate if pathogens persist in their invasion. This will be covered in detail in Chapter 12.
Body organisation and the immune system
The tube model of the body

A useful way to understand the body's organisation is to think of it as a hollow tube or pipe:
- The inside tunnel (lumen) represents the digestive system, which contains bacteria including both beneficial microflora and potential pathogens like E. coli
- The outside of the tube is exposed to environmental micro-organisms
- The tube wall itself represents the body's tissues, which must remain sterile
The entire defence system is dedicated to preventing micro-organisms from entering the tissue itself (the 'plastic' of the tube). Breach of this barrier can lead to serious systemic infections.
Sterile compartments
Certain internal compartments must remain free from microbial contamination:
- Thoracic cavity
- Cranial cavity
- Abdominal cavity
- Blood vessels of the cardiovascular system
If pathogens enter these sterile spaces, severe consequences may result. This is why a ruptured appendix or penetrating chest wound constitutes a medical emergency.
Components of the immune system
Antigens
An antigen is any molecule that the body recognises as foreign and that triggers an immune response.
- Body cells have 'marker' molecules on their surface identifying them as 'self'
- Pathogens have different chemical markers (antigens) recognised as 'non-self'
- Antigens can come from pathogens, foreign cells, cell fragments, protein debris, bacterial toxins, or snake venom
The lymphatic system
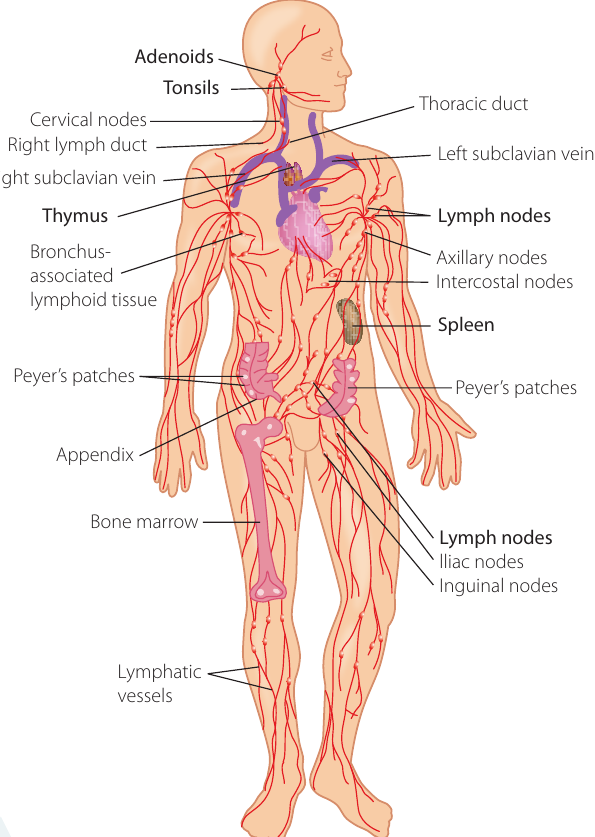
The lymphatic system plays a crucial role in the body's defence. It consists of:
- Lymph (milky fluid derived from tissue fluid)
- Lymph vessels (one-way drainage system)
- Lymph nodes (filter pathogens and debris)
- Lymphoid organs: thymus, spleen, tonsils, adenoids
Function: As blood circulates, plasma moves into tissues as tissue fluid, then enters lymph vessels. Lymph flows through lymph nodes where pathogens, cellular debris, and cancer cells are filtered out before the cleansed fluid returns to the blood via the thoracic duct.
Clinical significance: Swollen lymph nodes (glands) are a good indicator of the body's response to infection, as the drainage routes for particular lymph nodes are known. Doctors can often determine the infection site by which lymph nodes are swollen.

White blood cells (leucocytes)
White blood cells play pivotal roles in innate and adaptive immune responses. They differ in:
- Size
- Presence of granules in cytoplasm (granular or agranular)
- Colour of granules and cytoplasm (eosinophilic, basophilic)
- Shape of nucleus (lobed or mononuclear)
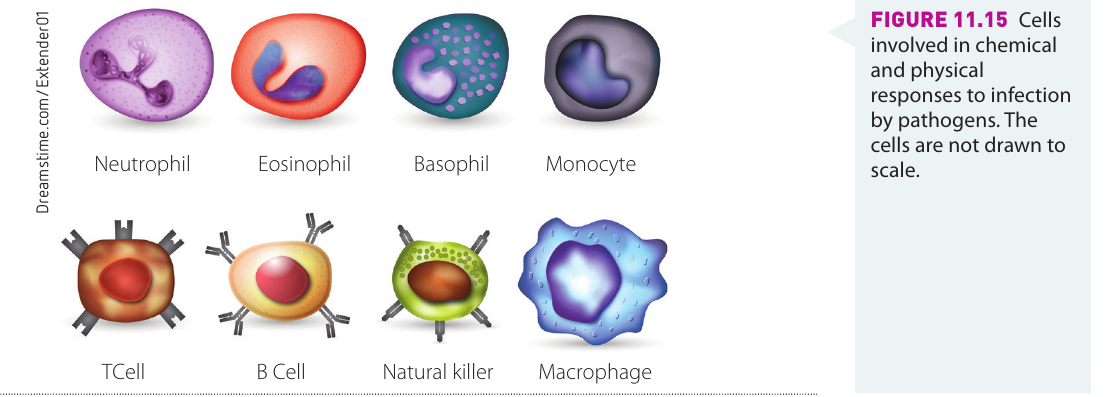
Major types of white blood cells and their functions:
| Cell Type | Characteristics | Location |
|---|---|---|
| Neutrophil | Most common at infection sites; releases toxins killing bacteria and fungi; recruits other immune cells | Migrates from blood vessels into tissues |
| Eosinophil | Releases toxins that kill bacteria and parasites | Circulates in blood, migrates to tissues |
| Basophil | Defends against parasites; releases histamines causing inflammation; involved in allergic reactions | Circulates in blood, migrates to tissues |
| Monocyte | Differentiates into dendritic cells and macrophages | Stored in spleen, moves through blood vessels to infected tissues |
| Macrophage | Phagocytosis of pathogens and cancer cells; antigen-presenting cell | Migrates from blood vessels into tissues |
| Natural killer cell | Kills tumour cells and virus-infected cells | Circulates in blood, migrates into tissues |
| Dendritic cell | Antigen-presenting cell; triggers adaptive immune response | Epithelial tissues; migrates to lymph nodes upon activation |
| Mast cell | Blood vessel dilation; releases heparin and histamines; recruits neutrophils and macrophages; involved in allergic reactions | Connective tissues and mucous membranes |
First line of defence
Physical barriers
Physical barriers make it difficult for pathogens to adhere to cells or penetrate tissues.
Routes of pathogen entry
Pathogens can enter the body through various routes:
Mucosal surfaces:
- Airway (inhaled droplets) - e.g., influenza, meningitis
- Gastrointestinal tract (contaminated water/food) - e.g., typhoid, diarrhoea
- Reproductive tract (physical contact) - e.g., syphilis
External epithelia:
- External surface (physical contact) - e.g., athlete's foot
- Wounds and abrasions - e.g., anthrax, tetanus
- Insect bites - e.g., yellow fever, Lyme disease, malaria
Skin
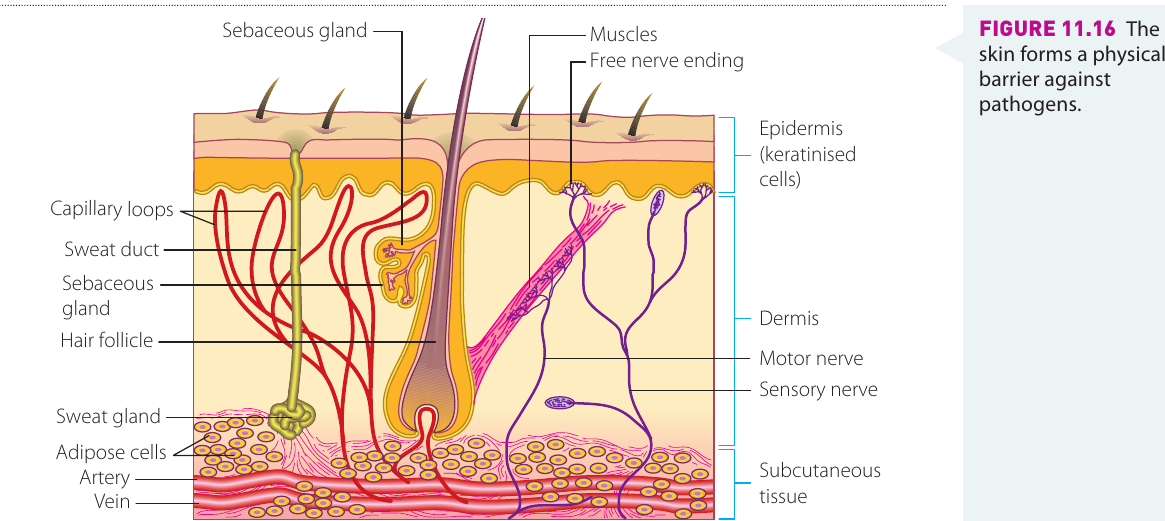
The skin consists of three layers:
- Epidermis (outer layer with keratinised cells)
- Dermis (underlying layer)
- Hypodermis (subcutaneous tissue)
Protective features:
- Keratin barrier: A waterproof protein secreted by keratinocytes that is mechanically tough and resistant to bacterial enzyme degradation
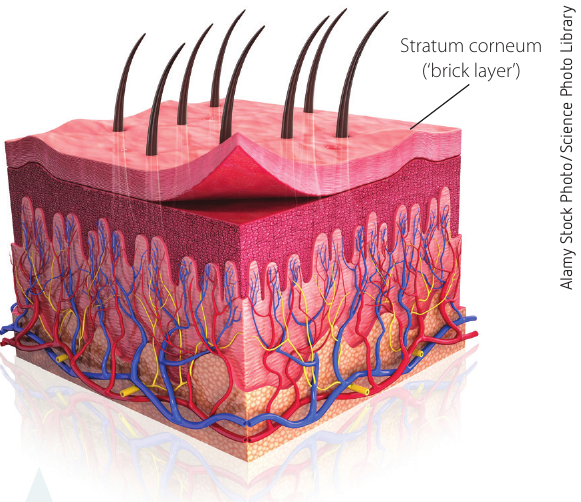
- Stratum corneum: Upper epidermal layer of flattened dead skin cells arranged in a 'bricks and mortar' structure, forming an effective physical barrier
- Exfoliation: Dead cells flake off, taking pathogens with them
- Blood supply: Provides early access for white blood cells, red blood cells, and platelets to wounds
Wound healing process:
- Inflammation - initial response to seal and protect
- Proliferation - new cells multiply rapidly to seal the wound
- Maturation - cells mature and complete the new barrier
Mucous membranes
Mucous membranes are moist pink tissues lining entry points to the body, including the mouth, nasal cavity, conjunctiva, and entrances to digestive and genitourinary systems.
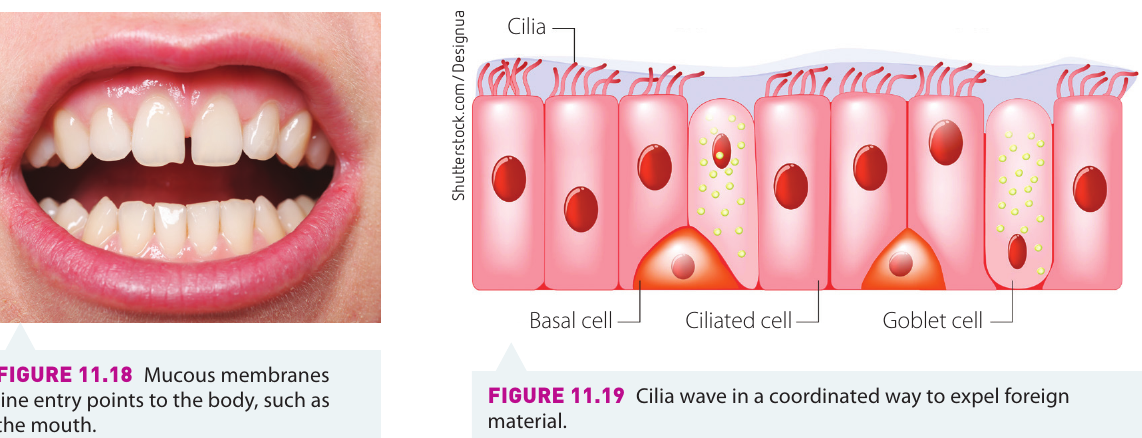
Protective features:
- Cell junctions anchor epithelial cells together, restricting pathogen access
- Cilia: Tiny hair-like structures that beat in coordinated waves to remove particles from the respiratory system (the muco-ciliary escalator)
- Constant cell renewal: Sheets of cells continuously grow upwards to replace surface cells lost to wear or pathogen attack
- Secretions: Mucus, lysozyme, and immunoglobulins (antibodies)
Tight junctions
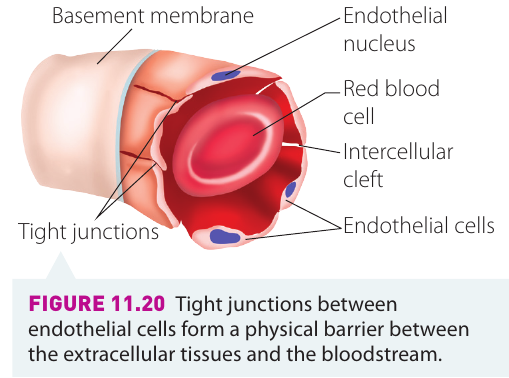
Blood vessels are lined internally by endothelial cells with tight junctions that prevent pathogen entry from infected tissue into the bloodstream.
- Bacteraemia: The presence of bacteria in the bloodstream (dangerous as bacteria can travel to distant sites)
- Blood-brain barrier: A particularly important example where brain endothelial cells connected by tight junctions restrict bacterial entry to the brain
The blood-brain barrier is crucial for protecting the central nervous system. Any breach of this barrier can lead to serious conditions such as meningitis or encephalitis.
Mucus
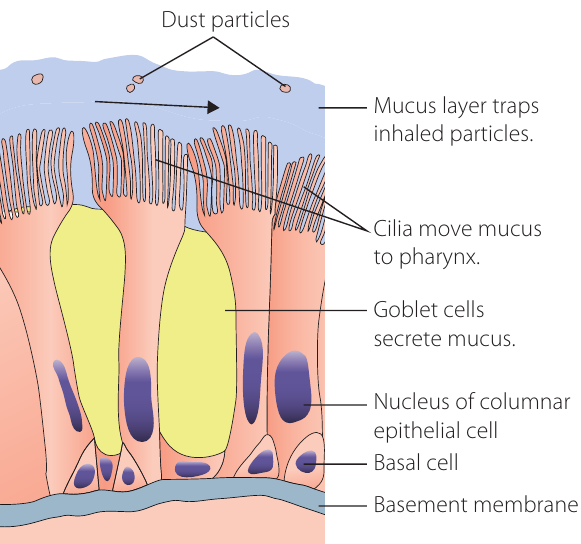
Mucus is a slippery substance secreted by goblet cells that line mucous membranes.
Functions:
- Traps foreign substances (pathogens, dust, pollen)
- Prevents pathogen entry through cells lining the alimentary canal
- Forms cervical mucus plugs guarding the uterus during pregnancy
- Contains substances inhibiting viral replication (e.g., against rotaviruses)
Clinical sign: Increased mucus production in the respiratory tract (runny nose, cough) indicates the body attempting to flush away pathogens. Green mucus indicates white blood cell activity.
Peristalsis
Peristalsis is the coordinated contraction of smooth muscle in the alimentary canal wall that moves food in one direction only.
Protective function: Prevents stasis (lack of movement) which could lead to bacterial overgrowth, as bacteria would have opportunity to proliferate.
Sphincters
A sphincter is a circular muscle maintaining constriction of a body passage, relaxing as required by normal physiological functioning.
Examples:
- Lower oesophageal sphincter (between oesophagus and stomach)
- Pyloric sphincter (between stomach and duodenum)
- Ileocaecal sphincter (between ileum and large intestine)
- Urethral sphincters (controlling urine release from bladder)
- Sphincter of Oddi (controlling digestive juice flow to duodenum)
Function: Help physically seal off compartments in the body to reduce pathogen invasion.
The microbiome: a natural barrier
The microbiome is the large and varied population of microbes living on the skin, in the intestines, colon, mouth, and vagina.
Protective mechanism: These natural microbes out-compete pathogenic ones, inhibiting their growth and multiplication.
Example: Candidiasis (thrush)
Candida albicans is a fungus normally present in low numbers on mucous membranes. If the microbiome balance is upset, C. albicans increases and causes disease.
Factors disrupting microbiome balance:
- Antibiotic use (reduces beneficial bacteria)
- Immune system suppression (inherited conditions, cancer treatment, HIV/AIDS)
- Diabetes mellitus (high sugar levels)
- Corticosteroid use
- Hormonal changes (pregnancy, oral contraceptives)
- General illness
- Intravenous drug use
Chemical barriers
Chemical barriers are non-specific substances secreted by epithelial tissue to prevent pathogen entry.
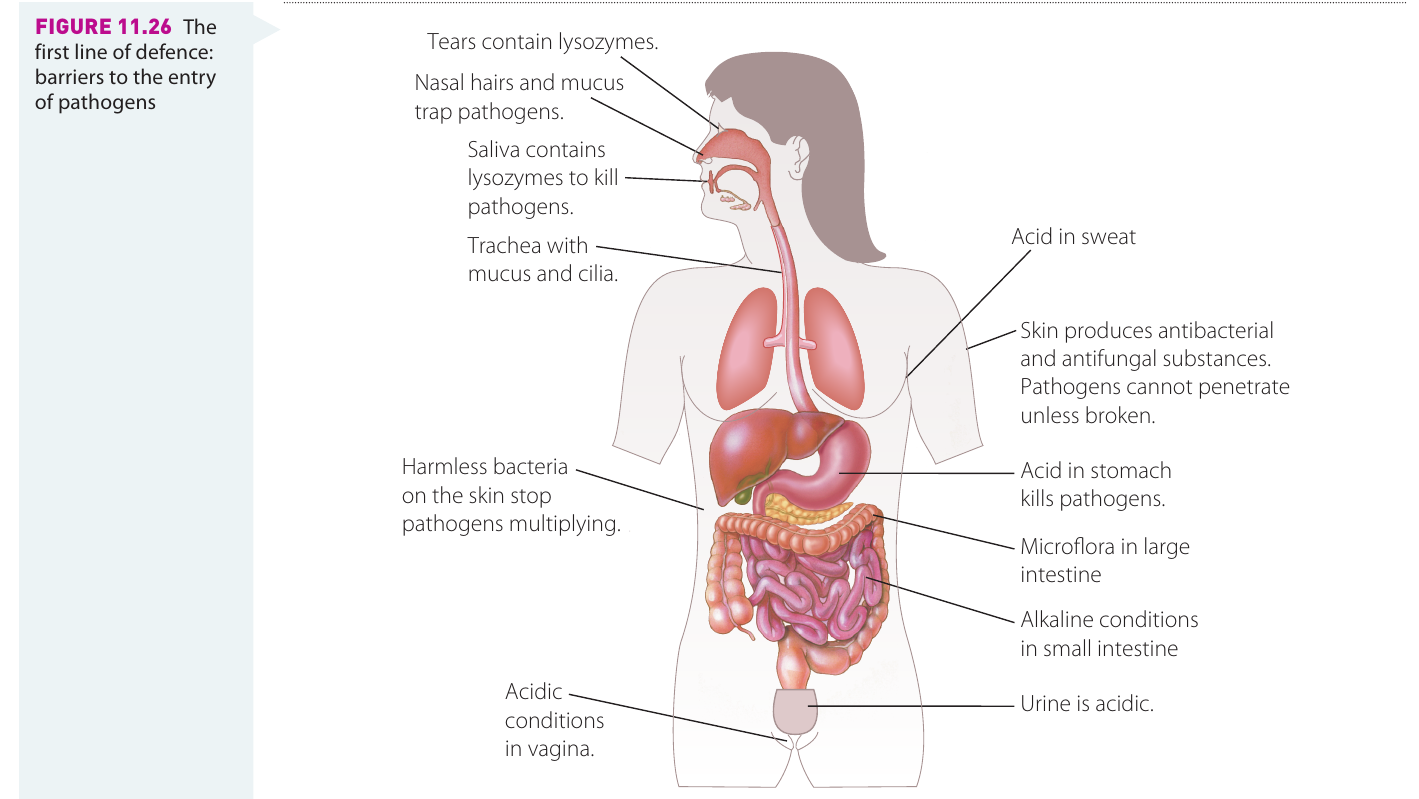
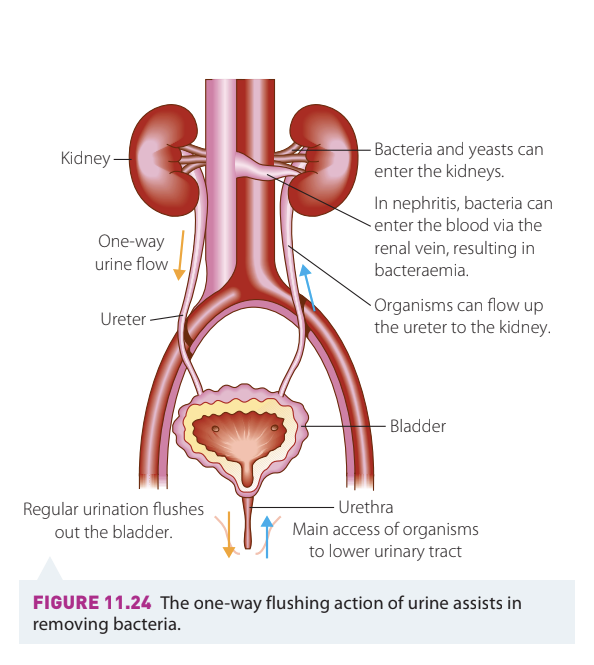
Urine
Urine is sterile until reaching the lower urethra. Females have shorter urethras than males and are at greater risk of urinary tract infections.
Chemical components defending against pathogens:
- Antimicrobial peptides (AMPs): Prevent bacterial binding to epithelial cells and break down bacterial cells
- pH: Normal human urine pH ranges from 4.5 to 8 (average 5-6, slightly acidic). Phagocytes work best in alkaline urine.
Physical defence: The flushing activity during urination (micturition) keeps pathogens away from the bladder.
Sebum and sweat
Sebum: Oily material secreted by sebaceous glands that waterproofs and lubricates skin.
Protective features:
- Skin pH around 5.5 (acidic) due to lactic acid, amino acids, and fatty acids
- Lysozyme secreted in perspiration breaks down bacterial cell walls
Saliva
Saliva is a complex mixture produced by salivary glands containing:
- Water and mucus
- Electrolytes
- Enzymes (e.g., amylase)
- Antimicrobial substances (lysozyme, immunoglobulin A (IgA), antimicrobial peptides)
Functions: Flushing action against microbes plus chemical activity through antimicrobial molecules.
Tears
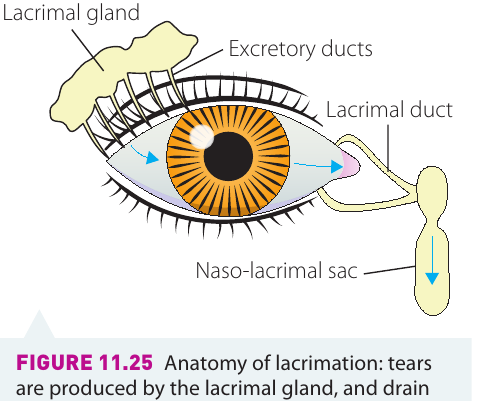
Lacrimation (tear production) occurs in lacrimal glands. The tear film covers the cornea and conjunctiva, containing:
- Lysozyme, lactoferrin, lipocalin
- Antimicrobial peptides (AMPs)
- Complement proteins
- Immunoglobulin A (IgA)
- Mucins (from goblet cells)
Gastric (stomach) secretions
Parietal cells lining the stomach wall secrete hydrochloric acid, creating a highly acidic environment (pH 1-2) that discourages microbial growth and survival.
Additional protection: The enzyme pepsin (from chief cells) plays an antimicrobial role.
Limitations: Many bacterial pathogens (E. coli, Salmonella typhimurium, Helicobacter pylori) have developed adaptive mechanisms to survive acidic conditions. Eating may raise stomach pH above the threshold needed to destroy bacteria.
pH change: As food moves to the duodenum, pH rapidly changes to around 6 due to highly basic bile, providing another limiting factor for pathogen growth.
Second line of defence
Physical responses to infection
Granuloma formation
When infected cells cannot be successfully defended, they may be surrounded by a wall of dead cells forming a capsule called a granuloma. This prevents infection spreading to other areas.
- Cells inside the granuloma die, destroying the pathogens infecting them
- Debris is destroyed by surrounding macrophages
- Typical of tuberculosis and leprosy (Mycobacterium spp.)
Vomiting and diarrhoea
Vomiting (emesis): A reflex action coordinated by the brain's vomiting centre in response to pathogens in the gut (gastroenteritis). The body's way of expelling harmful substances.
- Hypersalivation occurs before vomiting to protect tooth enamel from stomach acid
Diarrhoea: Rapidly expels micro-organisms from the gastrointestinal system.
While unpleasant, vomiting and diarrhoea are protective mechanisms. However, prolonged episodes can lead to dehydration and require medical attention.
Increased urination
When the bladder lining is attacked by a pathogen, the body responds with:
- Inflammation (cystitis)
- Pollakiuria (frequent passage of small amounts of urine)
This flushing response helps remove pathogens from the urinary tract.
Wound healing
When barriers are breached, the body's priorities are:
- Stop bleeding (haemostasis) - vasoconstriction, platelet plug formation, fibrin mesh, clot formation
- Confront pathogens - prevent infection
- Heal and repair - re-establish the barrier
The inflammatory response then begins.
Inflammation: a chemical response
Inflammation is a non-specific chemical response occurring at the site of infection that helps wound repair and pathogen destruction.
Five cardinal signs of inflammation
- Dolor (pain) - due to release of chemical mediators
- Calor (heat) - due to increased microcirculation
- Rubor (redness) - associated with increased microcirculation
- Tumor (swelling/oedema) - as fluids move from blood vessels to extracellular space
- Functio laesa (loss of function) - due to pain and swelling
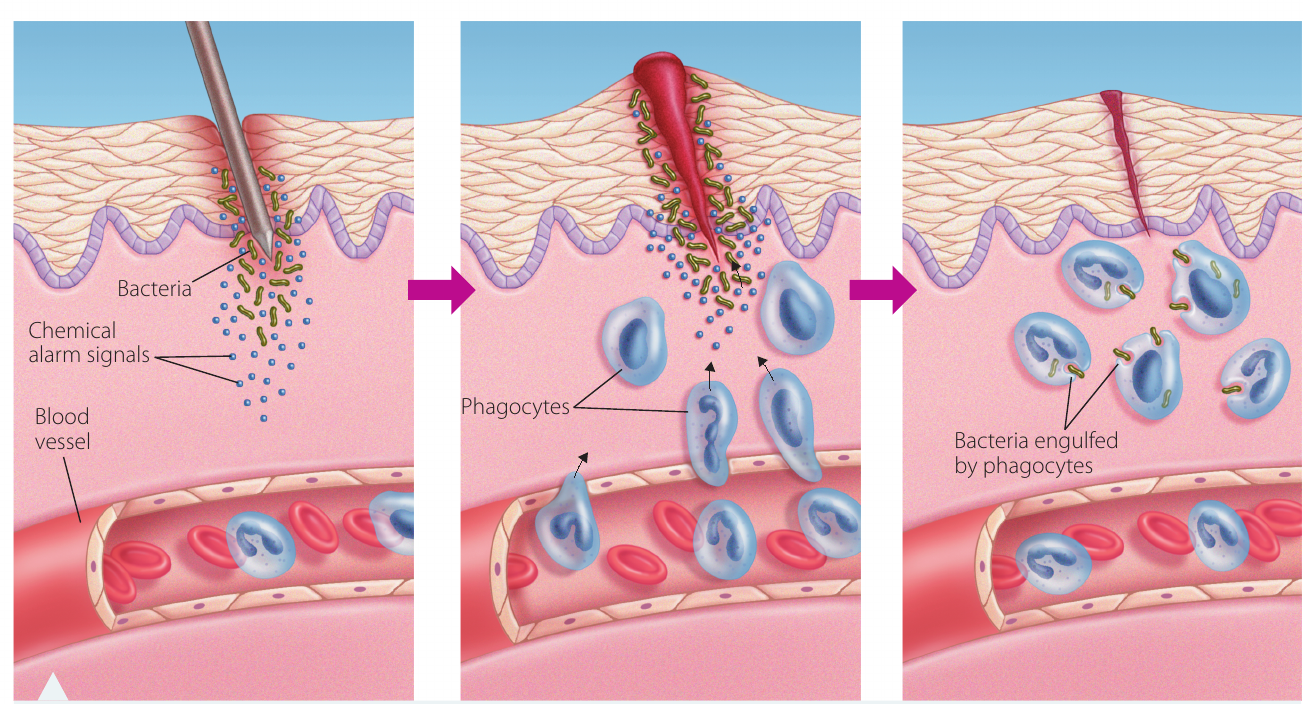
Mechanism of inflammation
When cells are challenged by pathogens or damaged:
- Chemical 'alarm signals' released: Histamines (trigger vasodilation and increase vascular permeability), bradykinin, serotonin, prostaglandins (associated with pain and fever)
- Capillaries dilate: Increased blood flow causes redness, heat, and swelling
- Increased vascular permeability: Allows white blood cells to move from blood into tissues
- Phagocyte recruitment: Attracted by chemotactic factors
- Temperature increase: Endogenous pyrogens released, inhibiting pathogen growth and increasing biochemical reaction rates
- Pathogen destruction and removal: Toxins removed, tissues repaired
Damage-associated molecular patterns (DAMPs) can initiate inflammation even when a wound is sterile (no pathogen present). This explains why injuries like cuts or burns become inflamed even in the absence of infection.
Phagocytosis: a cellular response
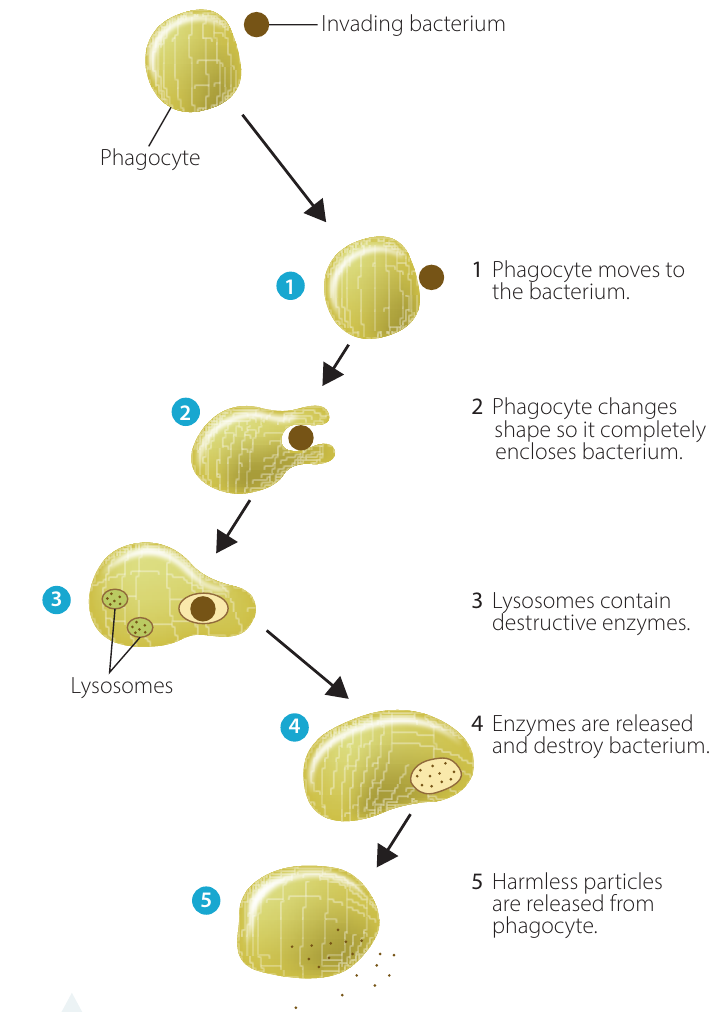
Phagocytosis is the process by which phagocytes change shape to surround and enclose foreign particles (e.g., bacteria), then release enzymes to destroy them.
Process:
- Phagocyte moves toward bacterium
- Phagocyte changes shape to completely enclose bacterium
- Lysosomes (containing destructive enzymes) approach
- Enzymes released to destroy bacterium
- Harmless particles released from phagocyte
Main types of phagocytes:
- Neutrophils
- Monocytes/macrophages
- Dendritic cells
- Natural killer cells
Limitations: Phagocytosis is not always successful - pathogens can sometimes repel phagocytes or escape before complete destruction. In severe infections, immature neutrophils show 'toxic changes' due to bacterial toxins circulating in the blood (septicaemia).
Neutrophils
Neutrophils originate in bone marrow and are the first phagocytes to move to infection sites.
Key features:
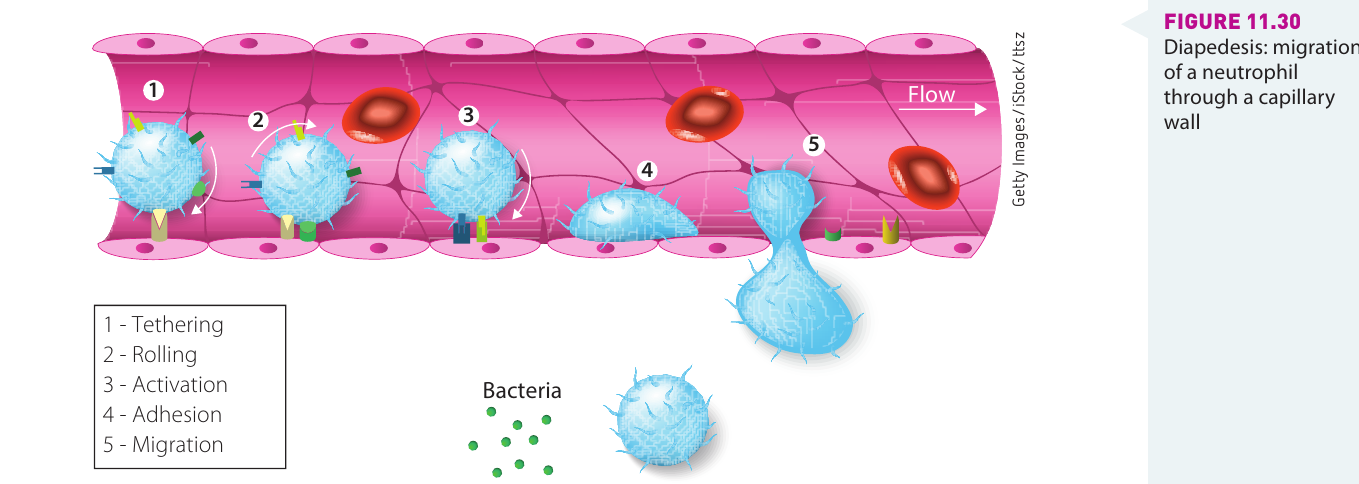
- Diapedesis: Can deform and squeeze between endothelial cells lining capillaries to move from blood to tissues
- Short-acting: Self-destruct after a few days
- Fight acute infections: Brief, severe infections
- Neutrophilia: Increased circulating neutrophils indicates active inflammation in the body
Destruction mechanism: Complex electron and ion flows create conditions in the phagocyte vacuole that kill microbes, which are then digested by enzymes (proteases).
Monocytes and macrophages
Monocytes circulate in blood until attracted to inflamed tissue, where they migrate through capillary walls and transform into:
- Macrophages ('big eaters') - long-lasting phagocytes fighting chronic infections
- Dendritic cells - antigen-presenting cells
- Osteoclasts - bone maintenance cells
Toll-like receptors (TLRs): On monocyte surfaces, recognise pathogen-associated molecular patterns (PAMPs) from bacterial cells.
Antigen presentation: After destroying foreign particles, macrophages and dendritic cells display parts of the antigen on their surface, acting as 'bridges' between innate and adaptive immune systems. This is crucial for activating the third line of defence.
The complement system
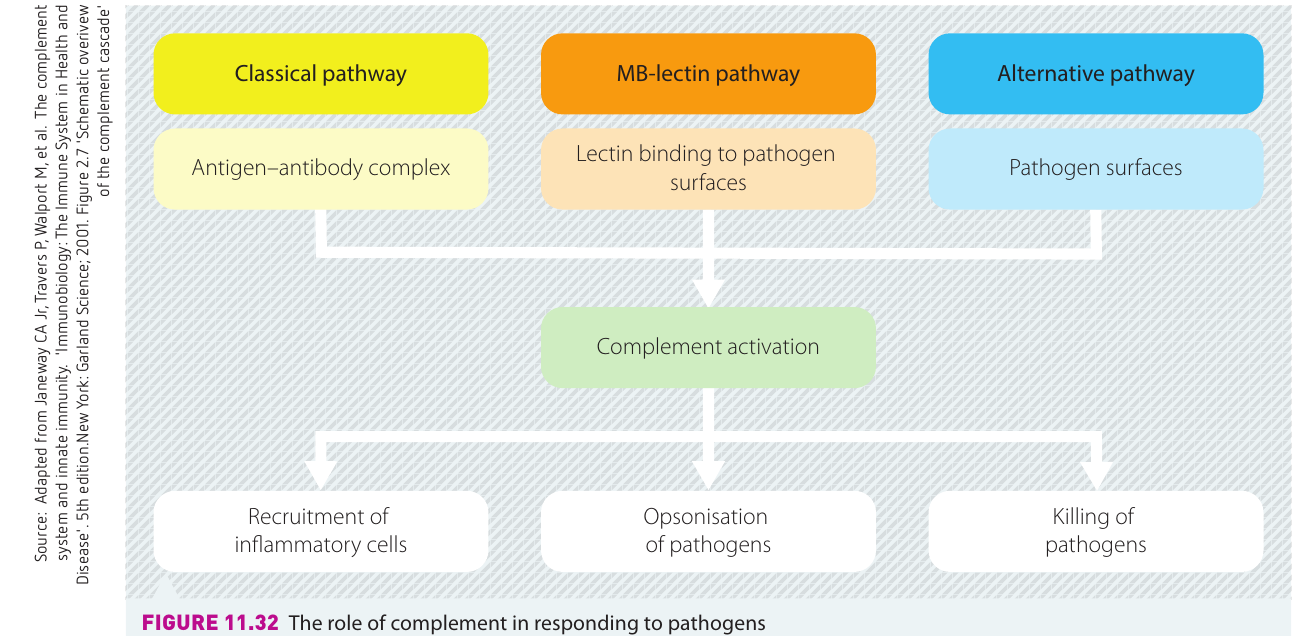
The complement system is a group of around 20 soluble proteins that assist other defence mechanisms in destroying extracellular pathogens.
Three activation pathways:
- Classical pathway - triggered by antigen-antibody complexes
- MB-lectin pathway - initiated by lectin binding to pathogen surfaces
- Alternative pathway - activated directly by pathogen surfaces
Functions:
- Stimulate phagocytes to become more active
- Attract phagocytes to infection sites (recruitment of inflammatory cells)
- Opsonisation - coating pathogens to enhance phagocytosis
- Destroy pathogen membranes (killing of pathogens)
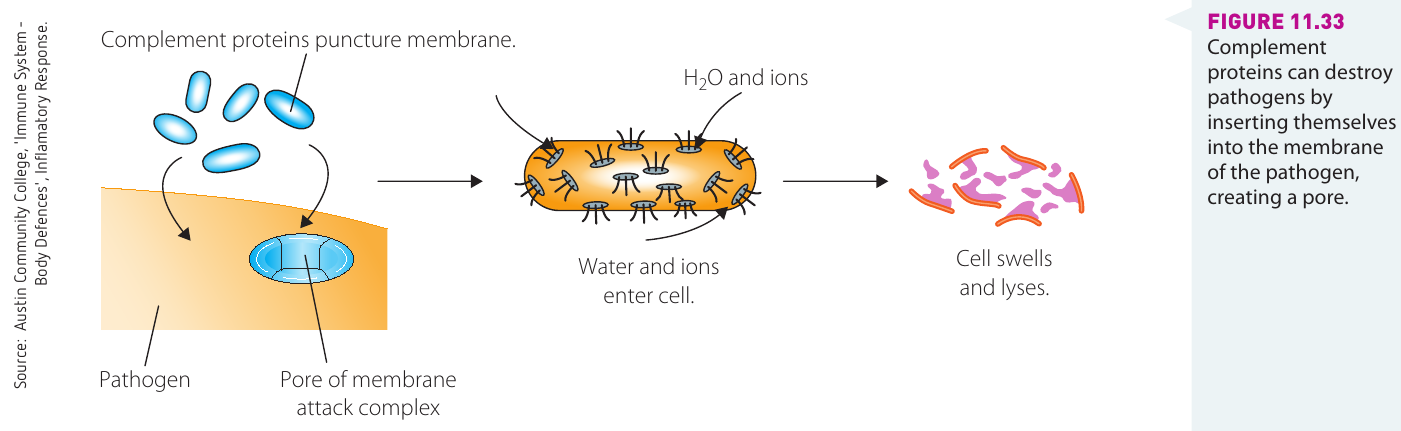
Membrane attack complex: Complement proteins insert into pathogen cell membrane, creating pores that allow water and ions to enter, causing cell swelling and lysis (bursting). This is a particularly effective mechanism against bacteria.
Fever: the role of pyrogens
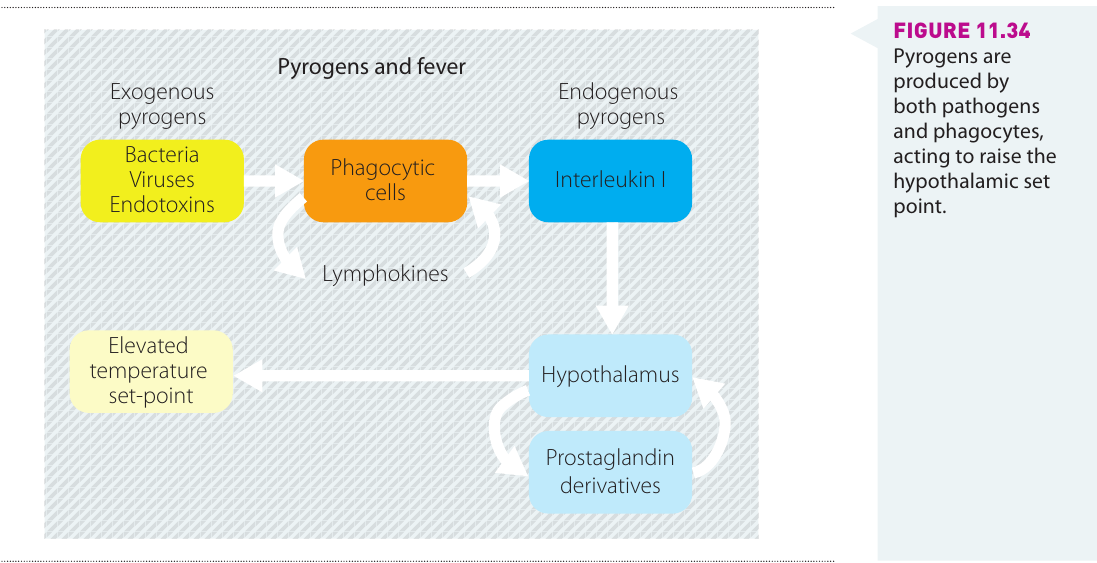
The hypothalamus in the brain regulates body temperature like a thermostat. Normal human body temperature averages 37°C.
Fever (pyrexia): Elevation of body temperature in response to pathogens.
Pyrogens ('fire starters'): Fever-causing chemicals
Two types:
- Exogenous pyrogens - from bacteria, viruses, endotoxins
- Endogenous pyrogens - from phagocytic cells (interleukin I), lymphokines
Mechanism: Pyrogens act on the hypothalamus → prostaglandin derivatives → elevated temperature set-point
Purpose:
- Kill or limit pathogen growth
- Enhance white blood cell activity
- Strengthen response to pathogens
Clinical considerations:
- Temporary mild fever (2-3 days) is normal and beneficial
- Very high fever for prolonged periods requires medical attention (may indicate significant illness, can cause seizures)
- Unexplained fever in children <3 months requires investigation, especially if child is listless, vomiting, or unresponsive
Cytokines
Cytokines are chemical messengers produced during infection that promote development and differentiation of T and B lymphocytes (third line of defence).
Examples:
- Interleukin (IL) - links innate and adaptive immune systems
- Interferons - signal viruses to stop replicating
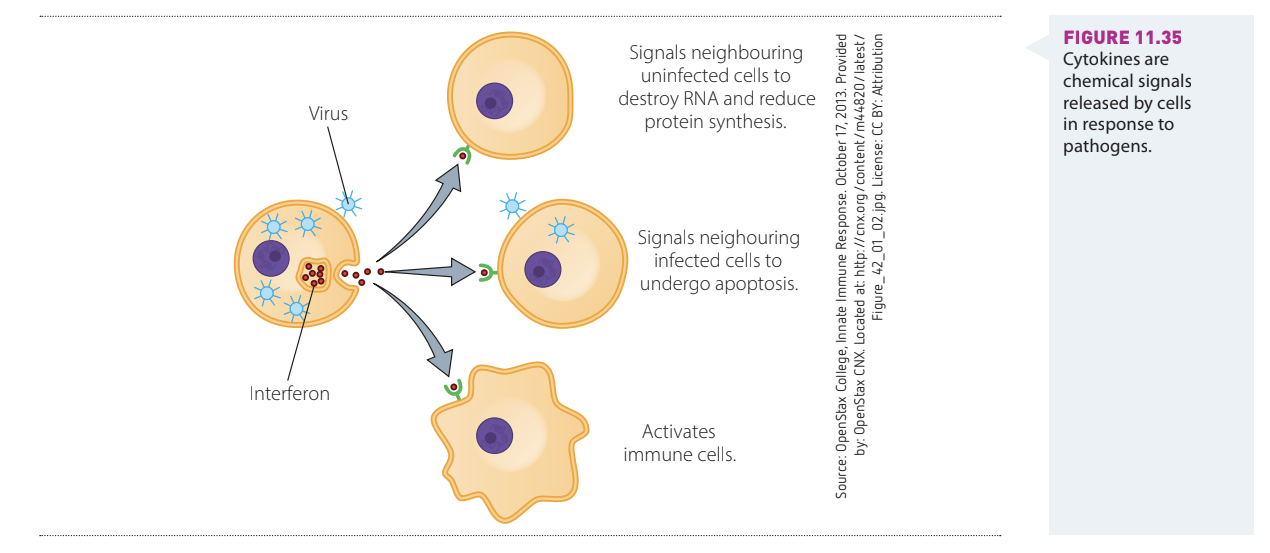
Interferon mechanism:
- Signals uninfected cells to destroy RNA and reduce protein synthesis
- Signals infected cells to undergo apoptosis (programmed cell death)
- Activates immune cells
Additional effects: Cytokines contribute to feelings of lethargy, muscle pain, and nausea during infection, causing the animal to isolate and rest, preventing spread to others. This is why you feel tired and want to sleep when sick!
Key Points to Remember:
-
The body has three lines of defence: First line (physical and chemical barriers), second line (inflammation and cellular responses), and third line (specific immune response)
-
Innate immunity is non-specific and present at birth, acting against any 'non-self' substance whether living or non-living
-
Physical barriers include: Skin with its keratin layer, mucous membranes with cilia, tight junctions between cells, sphincters, and the flushing actions of peristalsis and urination
-
Chemical barriers include: Acidic pH in urine, stomach, skin and vagina; antimicrobial substances in tears, saliva, sweat, and sebum; and the protective microbiome
-
The second line of defence involves inflammation, phagocytosis, fever, complement activation, and cytokine signalling - all coordinated chemical and cellular responses to pathogen invasion
-
White blood cells (neutrophils, macrophages, dendritic cells) are key players in detecting, engulfing, and destroying pathogens through phagocytosis and chemical signalling
-
The lymphatic system filters pathogens from tissue fluid and provides locations where immune responses can be coordinated