Tobacco, Alcohol, and Processed Foods (VCE SSCE Health and Human Development): Revision Notes
Tobacco, Alcohol, and Processed Foods
Introduction to globalisation and health
The modern world has experienced significant technological improvements that have reduced barriers to communication, trade, and transport. This has led to increased globalisation, which is the process whereby boundaries between countries are reduced or eliminated, allowing individuals, groups, and companies to act on a global scale. Globalisation can be described as transforming the different societies of the world into one global society.
Globalisation makes it easier for companies to distribute and market their products across the globe. Marketing refers to the activities of a company associated with selling a product or service, including advertising, selling, and delivering products to people.
While globalisation has enabled the distribution of beneficial products and services (such as certain pharmaceuticals and improved farming techniques) that can enhance health status, it has also facilitated the spread of harmful products including tobacco, alcohol, and processed foods. This demonstrates how the same process can have both positive and negative impacts on global health.
This note explores how the global distribution and marketing of these three products contribute to similarities and differences in health status and burden of disease between countries.
Tobacco
Targeting low- and middle-income countries
In recent decades, tobacco manufacturers have been actively targeting low- and middle-income countries in an attempt to compensate for lost revenue in high-income countries. Many high-income countries like Australia have implemented strict laws, taxes, regulations, and public awareness campaigns to reduce tobacco use. These interventions are often non-existent or less developed in low- and middle-income countries, making them attractive markets for tobacco companies.
As smoking rates have decreased in many high-income countries due to health interventions, tobacco companies have strategically increased their distribution and marketing efforts in low- and middle-income countries to maintain and grow global sales. This shift has had significant consequences for global health, transferring the burden of tobacco-related disease from wealthy to poorer nations.

Global statistics and trends
According to the World Health Organization (WHO), tobacco use is growing fastest in low-income countries. Currently, over 80 per cent of the world's 1.3 billion smokers live in low- and middle-income countries. This represents a dramatic concentration of tobacco use in regions that are least equipped to deal with its health consequences.
The future projections are even more concerning. It has been estimated that more than 80 per cent of the world's tobacco-related deaths will occur in low- and middle-income countries by 2030. This shift in the global burden of tobacco-related disease reflects the success of marketing efforts in these regions.
Gender differences in smoking
Smoking patterns vary significantly between males and females across different income groups. Traditionally, smoking has been considered a male activity in many cultures. However, tobacco companies have recognised this gap and invested heavily in advertising and promotional campaigns designed to tap into the female market, particularly in low- and middle-income countries.
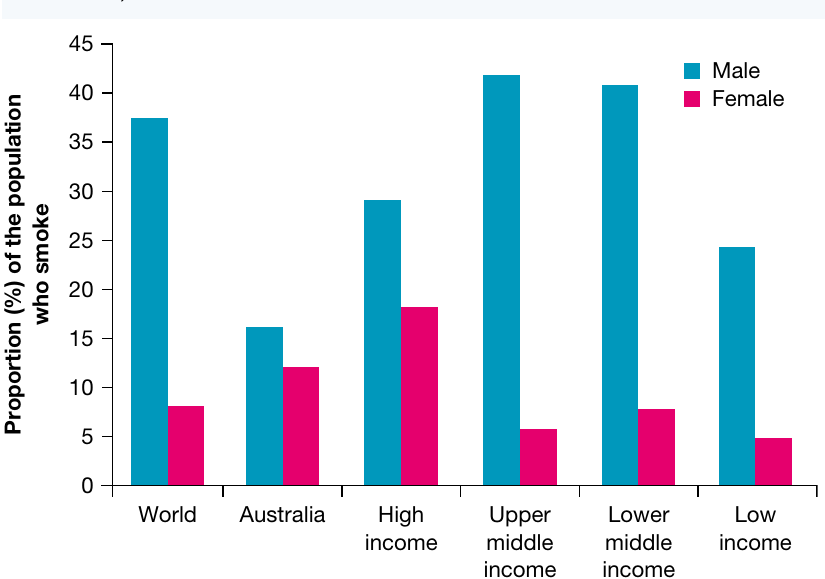
The data shows that males consistently have higher smoking rates than females across all income levels. Upper middle-income countries show the highest male smoking rate at around 42 per cent, while high-income countries show the highest female smoking rate at approximately 18 per cent. However, the concerning trend is the increasing rate of women smoking in low- and middle-income countries as a result of targeted marketing campaigns.
Children and tobacco
Children have also been influenced by advertising campaigns in low- and middle-income countries, and rates of children who smoke have increased. One factor that has contributed significantly to this trend is the ability to purchase single cigarettes in many low- and middle-income countries. This practice makes tobacco more affordable for those living in poverty, including children who have limited financial resources.
Australia's situation
In Australia, interventions by governments and non-government organisations have led to a decrease in smoking rates. These interventions include:
- Advertising and packaging laws (such as plain packaging)
- Increased taxation on cigarettes
- Laws restricting smoking in public places
- Public awareness campaigns about the health risks of smoking
Despite these improvements and the relatively lower smoking rates shown in the data, tobacco smoking remains a major health concern in Australia, similar to the situation in many low- and middle-income countries.
Impact on health status and burden of disease
The higher rates of smoking in low- and middle-income countries are contributing to an increased burden of disease, particularly through premature death. Many of these deaths result from:
- Cancer (particularly lung cancer)
- Cardiovascular disease
- Respiratory conditions
These are all directly associated with smoking.
Understanding Direct vs Indirect Health Impacts
Tobacco smoking affects health status and burden of disease in two key ways:
Direct impacts: Diseases caused by smoking itself, including cancer, cardiovascular disease, and respiratory conditions.
Indirect impacts: In low- and middle-income countries where financial resources are scarce, money spent on tobacco leaves less money available for essential items such as food, clothing, education, and basic healthcare. This creates a cycle where tobacco use increases the risk of conditions not necessarily caused by tobacco itself, such as infectious diseases. When families spend limited income on tobacco, they may not have sufficient resources to maintain proper nutrition, access healthcare, or provide education for their children.
Alcohol
Global consumption trends
Global alcohol consumption increased significantly in the 20 years leading up to 2010 and has remained fairly stable since then. However, the average amount of alcohol consumed across different income groups has changed considerably. Similar to tobacco companies, alcohol manufacturers have experienced a decrease in revenue in many high-income countries and are therefore increasingly marketing their products towards people in low- and middle-income countries.
Many alcohol producers would have neglected the low- and middle-income country market in the past, but these countries now provide them with an additional and growing source of income. Alcohol use is currently associated with about 3.5 per cent of global deaths, and the impact of alcohol use is predicted to increase in low- and middle-income countries if this trend continues.
Alcohol in Australia
Alcohol consumption is a significant concern in Australia, despite education and public awareness campaigns relating to alcohol misuse. The data shows that Australia's alcohol-related mortality rate is actually lower than the world average. However, it is important to note that the accessibility of healthcare in Australia may reduce the measurable impact of alcohol misuse compared with that in low- and middle-income countries.
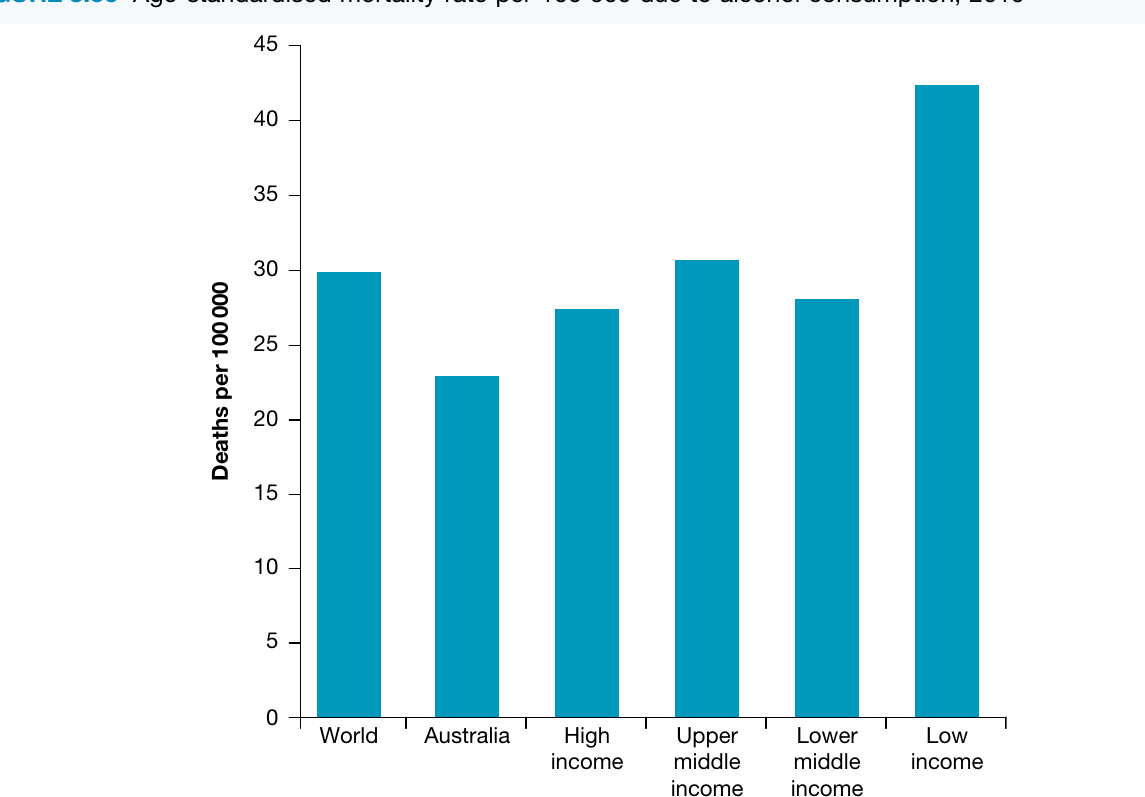
The chart shows that low-income countries have the highest age-standardised mortality rate from alcohol consumption at approximately 42 deaths per 100,000 population. Australia has one of the lowest rates at around 23 deaths per 100,000, while other income categories fall between 27 and 30 deaths per 100,000.
Impact on health status and burden of disease
Low- and middle-income countries experiencing an increase in alcohol consumption often face unique challenges. Many of these countries have no cultural relationship with alcohol consumption and lack the resources to:
- Educate the population about alcohol and its risks
- Control alcohol consumption through regulations
- Care for those suffering the negative effects associated with excessive drinking
Health conditions associated with alcohol misuse include:
- Liver disease
- Cardiovascular disease
- Cancer
Alcohol misuse can dominate people's lives, decreasing opportunities for them to lead healthy lives. People may prioritise alcohol over work, family responsibilities, and self-care, leading to a range of negative health and social outcomes. Similar to tobacco, if an individual's limited income is spent on alcohol, there may be less money available for food, clothing, shelter, and healthcare. This directly impacts the standard of living and increases the burden of disease through both direct effects of alcohol and indirect effects of poverty.
Processed foods
What are processed foods?
Processed foods are any food items that have been deliberately changed before being made available to eat. Food processing can range from very basic to highly complex:
- Basic processing includes drying or freezing food to maintain freshness
- Complex processing involves creating food items from a range of ingredients, such as jar pasta sauce, cake mix, or microwave meals
Not All Processed Foods Are Unhealthy
It is important to understand that many processed foods are healthy and safe to consume on a regular basis, such as:
- Canned fruit
- Frozen vegetables
- Dried beans
- Pasteurised milk
However, other processed foods contain significant amounts of added salt, sugar, and/or fat and should be consumed only sometimes and in small amounts, such as:
- Frozen pizzas
- Fast food hamburgers
- French fries (chips)
- Soft drinks
- Packaged snack foods
It is generally the unhealthier processed foods that are actively marketed to consumers and contribute to a range of negative health outcomes.
Global distribution and marketing
Companies producing processed foods have been marketing their products in low- and middle-income countries for many years. Several factors have increased both access to and consumption of processed foods in these countries:
- Increasing incomes, giving people more money to spend on convenience foods
- Migration of many people from rural areas to major cities, where processed foods are more available
- Aggressive marketing of these products

As a result of these trends, many people in low- and middle-income countries have neglected their traditional diets, which are often low in fat, in favour of westernised foods. These westernised foods are often high in fat, salt, and/or sugar and contribute to a more energy-dense diet.
Changes in food consumption
The following table shows how food consumption has changed over time and is projected to change in the future:
| Region | 1964–66 | 1974–76 | 1984–86 | 1997–99 | 2015 | 2030 |
|---|---|---|---|---|---|---|
| World | 9865 | 10,188 | 11,109 | 11,728 | 12,301 | 12,761 |
| Low- and middle-income countries | 8594 | 9004 | 10,251 | 11,217 | 11,924 | 12,468 |
| High-income countries | 12,330 | 12,824 | 13,414 | 14,142 | 14,403 | 14,644 |
Note: Values are in kJ per capita per day
This table shows that food consumption has increased across all regions over time. Importantly, low- and middle-income countries show a significant increase in per capita food consumption, rising from 8594 kJ per day in 1964–66 to a projected 12,468 kJ per day by 2030. While increased food availability can be positive, the concern is that much of this increase comes from unhealthy processed foods rather than nutritious whole foods.
Impact on health status and burden of disease
The increased consumption of unhealthy processed foods is contributing to an increased incidence of lifestyle diseases in low- and middle-income countries, including:
- Obesity
- Hypertension (high blood pressure)
- Cardiovascular disease
- Type 2 diabetes
Processed foods have been marketed in Australia for many years and have contributed to the high rates of overweight, obesity, and related conditions experienced in this country. According to the WHO, these causes of burden of disease are now on the rise in low- and middle-income countries as well.
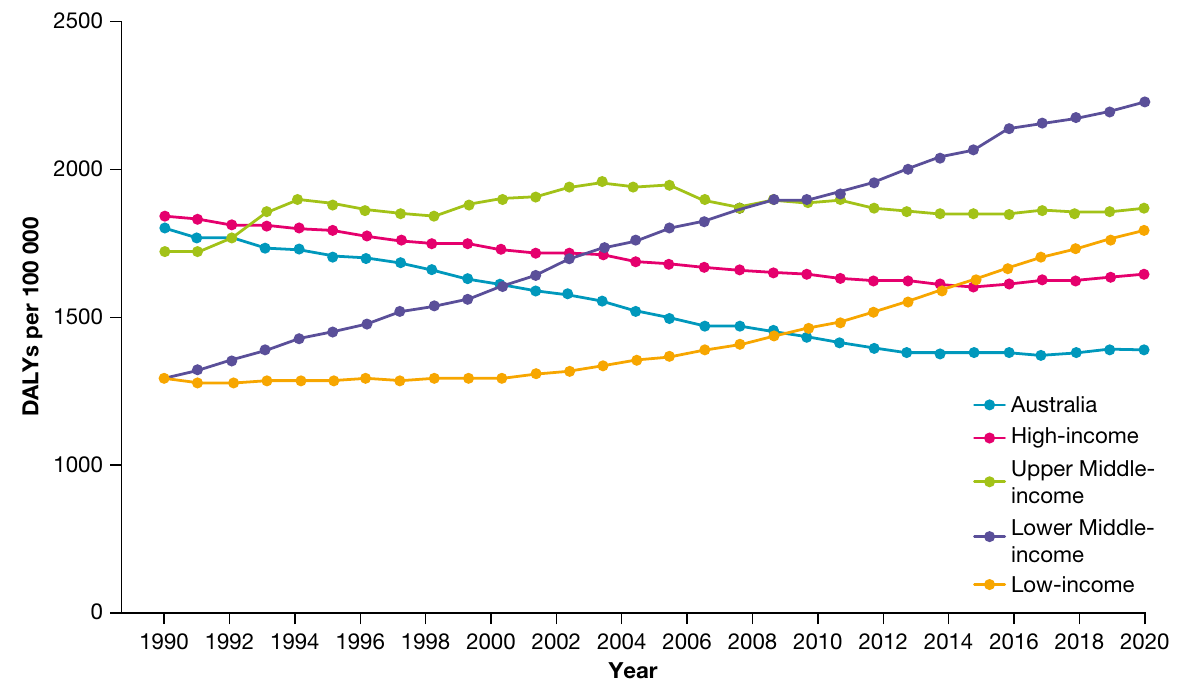
The graph shows how DALYs (Disability-Adjusted Life Years) per 100,000 people due to high body mass index have changed over time across different income groups. Lower middle-income countries show a dramatic increase from approximately 1250 DALYs per 100,000 in 1990 to over 2250 in 2020. This represents a substantial increase in the burden of disease related to obesity and overweight.
The rates of obesity among people of high socioeconomic status in countries like Brazil and India are now comparable with the United States and Australia. Higher rates of obesity result in higher rates of associated conditions including cardiovascular disease, hypertension, and diabetes. The WHO predicts the incidence of stroke deaths will double in low- and middle-income countries over the next 20 years. China is already experiencing the effects of westernised diets, with more than one million people dying of stroke each year. High salt intake is thought to be largely responsible for this trend.
The double burden of disease
The Double Burden of Disease
Many low- and middle-income countries now face a double burden of disease. This means they are experiencing:
- High rates of undernutrition and other conditions associated with poverty, such as infectious diseases
- Increasing rates of conditions associated with wealth, such as obesity and cardiovascular disease
Quite often, the effects of obesity and undernutrition exist side by side in the same community, or even in the same household. This creates complex challenges for health systems and policymakers, as limited resources must simultaneously address both poverty-related diseases and lifestyle diseases typically associated with wealth.
Chronic disease associated with a high intake of processed foods also impacts health status in other ways. For example, people with diabetes or cardiovascular disease may not be able to earn an income due to their illness. This reduces their standard of living and may further increase their risk of chronic illness and premature death, creating a vicious cycle.
Under-resourced health systems in many low- and middle-income countries mean that treatment for conditions related to obesity may not be available or affordable. This further contributes to mortality rates that are already higher than those in high-income countries.
Key Points to Remember:
-
Globalisation has reduced barriers to trade and communication, making it easier for companies to distribute and market products globally, including harmful products like tobacco, alcohol, and processed foods.
-
Over 80 per cent of the world's smokers live in low- and middle-income countries, where tobacco companies have increased marketing efforts. By 2030, over 80 per cent of tobacco-related deaths will occur in these countries.
-
Alcohol consumption is increasing in low- and middle-income countries due to marketing by manufacturers seeking new revenue sources. This contributes to increased mortality from liver disease, cardiovascular disease, and cancer.
-
The marketing of unhealthy processed foods in low- and middle-income countries is replacing traditional diets with westernised foods high in fat, salt, and sugar, contributing to increased rates of obesity, cardiovascular disease, and type 2 diabetes.
-
Many low- and middle-income countries face a double burden of disease, experiencing both undernutrition and poverty-related infectious diseases alongside increasing rates of obesity and chronic diseases associated with westernised lifestyles.
-
Both tobacco and alcohol spending can indirectly impact health by reducing money available for essential items like food, healthcare, and education, creating a cycle of poverty and disease.
-
Under-resourced health systems in low- and middle-income countries are struggling to address both traditional poverty-related diseases and emerging lifestyle diseases simultaneously.