Typical and Atypical Psychological Development (VCE SSCE Psychology): Revision Notes
Normal Variations in Brain Development
The origins of neurodiversity
The concept of neurodiversity emerged in the 1990s through the work of Australian sociologist Judy Singer. Whilst completing her honours degree at the University of Technology Sydney, Singer conducted pioneering sociological research into the social context surrounding autism spectrum disorders. Her research drew upon personal experiences across three generations of women on the autism spectrum and her involvement in establishing early online support groups for autistic individuals and their families.
Singer coined the term 'neurodiversity' with a specific political purpose: to argue for the recognition and acceptance of all neurotypes as valuable parts of human society. For Singer, neurodiversity refers to the limitless variation in human cognition and the uniqueness of each human brain. Although some critics have challenged neurodiversity as not being a scientific term, Singer maintains that this was never the intention. Rather, the term simply acknowledges the fundamental fact that no two human brains are identical.
Singer's work represented a significant shift in how society views neurological differences - moving from a deficit-based medical model to a diversity-based social model that recognises different brain types as normal human variations rather than disorders to be "fixed".
Understanding neurodiversity
Neurodiversity provides a framework for understanding why people think differently. This concept builds on the recognition that differences in thinking arise from both cultural and life experiences, as well as from the unique way each individual's brain is structured and functions. The neurodiversity approach suggests that diverse neurological conditions result from normal variations in the human genome, rather than representing defects or disorders.
A central principle of neurodiversity is the rejection of the idea that there exists one 'normal' or 'healthy' type of brain, or a single correct style of cognitive functioning. Instead, neurodiversity emphasises that every person possesses a unique nervous system with its own particular combination of abilities and needs. This represents an important shift away from viewing conditions like autism purely in terms of deficits and impairments. The neurodiversity perspective encourages a more positive view of such conditions as normal human differences, recognising that we all have distinctive combinations of strengths and challenges.
The neurodiversity framework challenges the traditional medical model by recognising that neurological differences are not inherently deficits. Every individual has a unique combination of strengths and challenges, and there is no single "correct" way for a brain to function.
The terminology surrounding neurodiversity includes the term 'neurodivergent', which refers to individuals whose brains function differently from the majority population (such as people with autism or ADHD). However, many individuals with these conditions prefer the term 'neurodiverse', which has developed as a positive descriptor that embraces differences in brain function and behaviour. The neurodiversity umbrella encompasses various conditions including autism spectrum disorder, ADHD, dyslexia, dyspraxia, and numerous other neurodevelopmental differences.
Autism spectrum disorder
Autism spectrum disorder represents a persistent neurodevelopmental condition characterised by symptoms that manifest from early childhood. According to the Australian Institute of Health and Welfare, ASD involves a cluster of characteristics related to social communication and behavioural patterns. Individuals with autism typically demonstrate difficulties with communication and social interaction across various contexts, both familiar and unfamiliar. These challenges manifest in several ways.
People with autism often struggle to understand emotional and social cues. This difficulty exists on a continuum, ranging from challenges maintaining typical conversations to complete inability to respond to social interactions or share emotions. In severe cases, individuals may be non-verbal. Non-verbal communication presents particular challenges, including:
- Lack of eye contact
- Inappropriate use of gestures or difficulty understanding them
- Reduced facial expressions
Additionally, forming and maintaining relationships proves difficult for many autistic individuals, encompassing challenges adjusting behaviour for different social contexts, making friends, and showing interest in peers.
Severity levels in autism
Once diagnosed, individuals with autism are classified according to the severity of their symptoms across two main domains: social communication impairments and restrictive, repetitive patterns of behaviour. This classification determines the level of support required and helps guide appropriate interventions.
The three severity levels are not fixed categories - an individual's support needs may change over time or vary across different contexts. The classification helps ensure appropriate support is provided based on current functioning.
Level 1 (Mild - requiring support): Individuals at this level show noticeable communication impairment when supports are not in place. They experience some difficulty initiating and responding to social interactions, show decreased interest in social interactions, and struggle to make friends. While they can speak in full sentences, their conversational exchanges with others appear atypical. Their inability to adapt behaviour inhibits functioning in certain situations. These individuals experience distress when switching between activities and struggle with organisation and planning, which affects their independence.
Level 2 (Moderate - requiring substantial support): At this level, individuals demonstrate noticeable impairment of verbal and non-verbal communication and social skills, even when support is available. They show limited initiation of or response to social interactions and speak in simple sentences. Their inability to adapt behaviour noticeably affects normal functioning across various situations. They experience difficulty coping with change and some difficulty or distress when changing focus or action.
Level 3 (Severe - requiring very substantial support): Individuals at this most severe level experience severe impairment of both verbal and non-verbal communication. They do not initiate or respond to social interactions except for specific wants or needs. They speak very little and often unclearly. Their restricted and repetitive behaviour prevents normal functioning. They do not cope well with change, and attempts to change their focus cause considerable distress.
Prevalence and causes of autism
In 2018, Autism Spectrum Australia estimated that approximately 1 in 70 Australians are autistic, equating to around 353,880 people. Autism is most frequently identified in children aged 3-14 years, with 83% of diagnoses occurring before age 25. The causes of autism are complex and multifaceted, involving various genetic and environmental factors. The condition often co-occurs with other neurological or mental conditions, such as epilepsy and ADHD.
Common Misconception: Many people expect to see clear structural differences between autistic and neurotypical brains. However, the differences between any two neurotypical brains are often more dramatic than the subtle differences associated with autism. Brain structure alone cannot be used for diagnosis, as there is considerable variability throughout the human nervous system.
Whilst neuroimaging techniques enable researchers to observe and measure structural and functional differences in the brain, distinguishing an autistic brain from a neurotypical brain remains challenging. Many of the differences are subtle and emerge from studies that have averaged findings across large numbers of individuals. Remarkably, the differences between the brains of two neurotypical individuals are often more dramatic than the subtle brain differences associated with autism. Furthermore, some structural differences observed in people with autism also appear in brain scans of neurotypical individuals and those with other neurodevelopmental conditions, such as ADHD. This overlap highlights the considerable variability and diversity that exists throughout the human nervous system. Consequently, the brain itself cannot indicate clear-cut causes and cannot be used conclusively in diagnosis.
Cognitive variations in autism
Rather than focusing on structural brain differences, it proves more helpful to compare the cognitive variations between neurodiverse individuals with autism and neurotypical individuals. Three key cognitive variations are consistently observed in autism: differences in theory of mind, executive function, and central coherence.
Remember "TEC": The three key cognitive variations in autism are:
- Theory of mind
- Executive function
- Central coherence
This mnemonic can help you recall the main cognitive differences observed in autism.
Theory of mind
Theory of mind represents a cognitive ability that enables us to make judgements about other people's mental states. This ability typically develops in children between the ages of three and five. It allows us to use our understanding of others' beliefs, intentions, and desires to predict their behaviour. This capacity is essential for successful social interaction and communication.
Multiple studies have established that individuals with autism spectrum disorder demonstrate impaired theory of mind. Baron-Cohen, Leslie, and Frith's influential 1985 study used the Sally-Anne test to evaluate theory of mind in both neurotypical children and neurodiverse children with autism spectrum disorder or Down syndrome.
The Sally-Anne Test: Assessing Theory of Mind
The Sally-Anne test is a classic experiment used to assess whether children understand that others can hold false beliefs - a key component of theory of mind.
The Setup:
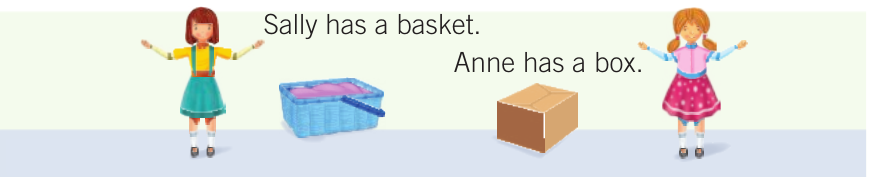
The child observes Sally placing her marble in her basket, with Anne also present in the scene.
The Action:

Sally then leaves the room.

While Sally is away, Anne moves the marble from Sally's basket to her own box.

The Test: When Sally returns, the child is asked three questions:
- Where will Sally look for her marble? (The belief question - the critical assessment)
- Where is the marble really? (The reality question - control)
- Where was the marble at the beginning? (The memory question - control)
Understanding the Results:
- Correct response: Pointing to the basket shows the child understands Sally has a false belief about where the marble is
- Pointing to the box indicates the child hasn't developed theory of mind - they assume Sally knows what they know
Baron-Cohen and colleagues found that 85% of the neurotypical children and those with Down syndrome correctly answered the belief question. In stark contrast, only 20% of the autistic children answered correctly, with the remaining 80% pointing to the actual location of the marble. Further research has revealed that neurotypical four-year-olds tend to have developed theory of mind and understand that Sally will look in the basket, whereas three-year-olds typically point to the box. This suggests that by age four, children have developed an understanding that other people possess different knowledge from them, enabling them to adjust their behaviour accordingly.
The cognitive ability to infer the mental states of others appears vital for the development of social communication. This may provide a cognitive explanation for why autistic children struggle with social communication - their delayed or absent development of theory of mind means they find it difficult to understand others' perspectives, beliefs, and intentions.
Executive function
Executive function represents a cognitive process that helps us set goals, organise and plan, focus our attention, and ultimately accomplish tasks. Executive functioning encompasses complex cognitive processes including working memory, problem-solving, and flexible thinking.
Research has established a relationship between executive dysfunction and both the social and non-social symptoms associated with autism. For example, children with autism typically score worse than neurotypical children on tests measuring short-term memory, mental processing speed, and impulse control. Additionally, they tend to prioritise accuracy over speed on reaction time tests, whereas neurotypical children balance accuracy with speed. These executive function differences help explain many of the daily challenges faced by individuals with autism, including difficulties with organisation, planning, and adapting to change.
Central coherence
Central coherence refers to a person's ability to derive overall meaning from a mass of details. An individual with strong central coherence, when viewing an endless expanse of trees, would perceive it as a 'forest'. Conversely, a person with weak central coherence would see only a large number of individual trees.
The 'weak central coherence theory', developed by Frith in 1989, proposes that people with autism possess a particular cognitive style that leads them to focus on details rather than the global idea. In other words, they struggle to see the bigger picture and instead become absorbed in the details, which can cause them to miss broader meaning.
Weak Central Coherence: A Strength and a Challenge
While weak central coherence can make it difficult for individuals with autism to understand overall context and meaning, this cognitive variation also represents a significant strength. The ability to focus intensely on fine details and extract them from complex data can be highly advantageous in fields such as:
- Mathematics
- Engineering
- Data analysis
- Quality control
- Research
This demonstrates how the same cognitive variation can function as both a deficit and an asset, depending on the context and demands of the situation.
However, this cognitive variation represents both a challenge and a potential strength. Some individuals with autism benefit from their ability to focus on fine details and extract these from complex data, which is recognised as an advantage associated with the condition. For instance, people with autism may excel in disciplines such as mathematics or engineering, where attention to detail is extremely valuable. Therefore, the weak central coherence observed in people with autism can function as both a deficit and a strength, depending on the context.
Attention deficit hyperactivity disorder
ADHD represents a neurodevelopmental disorder that affects some areas of brain function. The condition affects approximately one in 20 Australians - roughly one million people - yet remains frequently misunderstood and underdiagnosed. Key symptoms of the disorder include inattention, distractibility, hyperactivity, and impulsivity.

ADHD is diagnosed using the criteria outlined in the DSM-5-TR. For an ADHD diagnosis to be made, the symptoms of inattention (such as difficulty concentrating, forgetting instructions, and moving from one task to another without completing anything) and/or hyperactivity and impulsivity (such as talking over others, having a short temper, and being accident-prone) must meet several specific criteria:
- The symptoms need to be excessive for the developmental age of the individual
- Must have been present before the age of 12
- Must have persisted for longer than six months
- Must contribute to impairment across multiple settings such as home, school, childcare, or work
ADHD diagnosis requires careful assessment across multiple contexts. The symptoms must be persistent, developmentally inappropriate, and cause significant impairment in daily functioning. This ensures that typical childhood behaviours or temporary difficulties are not misdiagnosed as ADHD.
Cognitive variations in ADHD
Although many studies have reported brain structural differences in individuals with ADHD, researchers have not yet reached consensus on these findings. Nevertheless, several cognitive variations are known to occur in individuals with ADHD. These include, but are not limited to, differences in executive functioning, working memory, arousal and alertness, and time estimation.
Remember "EWAT": The four key cognitive variations in ADHD are:
- Executive function
- Working memory
- Arousal and alertness
- Time estimation
This mnemonic can help you recall the main cognitive differences observed in ADHD.
Executive function in ADHD
Similar to autism, individuals with ADHD experience deficits in executive function. These deficits affect multiple aspects of daily functioning, including:
- Organising, prioritising, and activating tasks
- Focusing, sustaining, and shifting attention to tasks
- Regulating alertness, sustaining effort, and processing speed
- Managing frustration and modulating emotions
- Using working memory
- Accessing recall
These executive function difficulties result in ADHD affecting a person's ability to self-regulate. This occurs because executive functions normally enable a person to control their thoughts, words, actions, and emotions. Executive function also helps us perceive and manage time, and direct and manage our behaviour over time.
Developmental Delay in ADHD:
In neurotypical children, executive functioning abilities develop sequentially from around age 2, with full development achieved at around age 30. In neurodiverse children with ADHD, these skills are delayed by approximately 30%, or three to six years.
Furthermore, most individuals with ADHD only develop up to 75-80% of the executive functioning capacity of their neurotypical peers, meaning that this lag continues throughout life. This permanent developmental difference has significant implications for expectations, support needs, and understanding the challenges faced by individuals with ADHD across their lifespan.
In neurotypical children, executive functioning abilities develop sequentially, with each new skill building on previous ones. This development usually begins at around two years old, with full development achieved at around age 30. In neurodiverse children with ADHD, these skills are delayed by approximately 30%, or three to six years. Furthermore, most individuals with ADHD only develop up to 75-80% of the executive functioning capacity of their neurotypical peers, meaning that this lag continues throughout life.
Working memory
Individuals with ADHD experience dysfunctions in their working memory. Working memory represents the type of memory that allows us to process incoming sensory information. For this reason, people with ADHD can experience difficulty dealing with visual and spatial information and/or processing auditory information. These working memory challenges can manifest as:
- Difficulties following multi-step instructions
- Remembering information whilst working on a task
- Keeping track of multiple pieces of information simultaneously
Working memory challenges in ADHD explain why individuals may struggle with tasks that require holding and manipulating information in mind, such as mental arithmetic, following complex directions, or keeping track of conversations with multiple topics.
Arousal and alertness
Alertness refers to the ability to be vigilant and to sustain focus. Children with ADHD tend to be under-alert or experience problems with alertness. For instance, individuals with ADHD are more likely to respond quickly and carelessly to tasks, indicating a tendency to act impulsively. This impulsivity then interferes with learning or achievement, as they may complete tasks without sufficient thought or attention to detail.
Time estimation
Individuals with ADHD show variations in how they estimate time. Specifically, in contexts where time judgement is relevant to learning or decision-making, individuals with ADHD tend to overestimate even very short time intervals. This difficulty with time perception can contribute to challenges with planning, organisation, and meeting deadlines.
Key Points to Remember:
Neurodiversity Framework:
- Neurodiversity emphasises that there is no single 'normal' brain type; all neurological differences represent normal human variation
- The concept was pioneered by Judy Singer in the 1990s to promote acceptance of all neurotypes as valuable parts of society
- Terms like 'neurodivergent' and 'neurodiverse' describe individuals whose brains function differently from the majority population
Autism Spectrum Disorder:
- Characterised by difficulties with social communication and restrictive, repetitive behaviours
- Classified into three severity levels (mild, moderate, severe) based on support needs
- Affects approximately 1 in 70 Australians
- Three key cognitive variations: "TEC"
- Theory of mind: Impaired ability to understand others' mental states (demonstrated by Sally-Anne test)
- Executive function: Challenges with organisation, planning, and adapting to change
- Central coherence: Focus on details rather than the bigger picture (can be both strength and challenge)
Attention Deficit Hyperactivity Disorder:
- Affects approximately 1 in 20 Australians (around one million people)
- Key symptoms include inattention, hyperactivity, and impulsivity
- Diagnosis requires symptoms present before age 12, persisting for 6+ months, and causing impairment across multiple settings
- Four key cognitive variations: "EWAT"
- Executive function: Delayed by 3-6 years, with only 75-80% capacity of neurotypical peers throughout life
- Working memory: Difficulties processing and holding information
- Alertness: Tendency to be under-alert, leading to impulsive responses
- Time estimation: Tendency to overestimate even short time intervals
Important Distinction:
- Brain structure alone cannot diagnose autism or ADHD - the variability between any two brains is often greater than the differences associated with these conditions
- Focus on cognitive variations and functional impacts provides more helpful understanding than structural brain differences