Disease Prevention (OCR A-Level Biology A): Revision Notes
Defences Against Infection in Animals
Overview of defence mechanisms
Vertebrate animals possess sophisticated defence systems against pathogenic invasion. The body employs four principal defensive strategies:
- Physical defences: Structural barriers such as skin and mucous membranes that prevent pathogen penetration
- Cellular defences: Specialised cells that detect, ingest, and destroy pathogens
- Chemical defences: Secreted substances that create hostile environments for microorganisms or prevent their replication
- Commensal organisms: Harmless bacteria and fungi that compete with pathogens, preventing colonisation
These strategies operate across three interconnected lines of defence, each combining cellular and chemical components to protect against infection.
The three lines of defence work together as an integrated system, with each line providing backup when the previous line is breached. The first line prevents entry, the second line responds rapidly to invasion, and the third line provides targeted, long-term protection.
First line of defence
The first line of defence comprises physical and chemical barriers that prevent pathogen entry into the body. These mechanisms operate continuously and non-specifically.
Key term: First line of defence – Physical and chemical defences that prevent pathogen entry, including skin, mucous membranes, and antimicrobial secretions such as lysozyme, sebum, and hydrochloric acid.
Physical barriers
The skin forms an effective barrier through its outer layer of dead, keratinised cells. Keratin is a tough, fibrous protein that creates a relatively dry, acidic surface with high salt content (from evaporated sweat). These conditions inhibit microbial growth and multiplication.
Mucous membranes line internal surfaces including the alimentary canal, respiratory tract, and urinogenital system. These membranes consist of epithelial cells interspersed with mucus-secreting cells such as goblet cells.
Mucus contains glycoprotein molecules with extensive carbohydrate chains, creating a sticky substance that traps particulate matter including bacteria, viruses, dust, and pollen. In the respiratory tract, cilia move this trapped material upwards towards the throat for expulsion.
The combination of mucus production and ciliary action is particularly important in the respiratory system, where it forms the mucociliary escalator. This continuous upward movement helps clear the airways of trapped pathogens and debris, reducing the risk of respiratory infections.
Expulsive reflexes
When pathogens irritate airway linings, they trigger expulsive reflexes – sudden expulsions of air that eject foreign particles from the upper respiratory tract. Coughing and sneezing remove secretions containing trapped pathogens, though this mechanism may also facilitate pathogen transmission.
Key term: Expulsive reflex – Coughing and sneezing that expel irritants (potentially including pathogens) from the upper gas exchange system, throat, and nasal passages.
Chemical defences
Several antimicrobial chemicals contribute to first-line defence:
- Lysozyme: An enzyme secreted into body fluids (blood, sweat, tears, milk) that catalyses bacterial cell wall breakdown
- Fatty acids: Present in sebum secreted onto skin surfaces, possessing antimicrobial properties
- Hydrochloric acid: Secreted by stomach lining cells, kills bacteria ingested with food
- Mucus: Secreted along the gut length to protect against acid, enzymes, and pathogens
Lysozyme is particularly effective against Gram-positive bacteria because it targets peptidoglycan in their cell walls. This enzyme is found in high concentrations in tears, making the eyes particularly well-protected against bacterial infection.
Commensal organisms
The body hosts numerous non-pathogenic microorganisms, including Candida albicans (yeast) and Escherichia coli (bacteria). These organisms inhabit the skin, mouth, intestines, and other body regions without causing disease.
E. coli in the large intestine forms part of the normal intestinal flora. These commensal organisms benefit the host by competing with pathogenic species, preventing their establishment. When commensal growth is suppressed (e.g. during antibiotic treatment), opportunistic pathogens may infect and cause disease.
The disruption of commensal organisms during broad-spectrum antibiotic treatment can lead to secondary infections by opportunistic pathogens. This is why patients taking antibiotics sometimes develop conditions like thrush (Candida albicans overgrowth) or Clostridium difficile infections in the gut.
Limitations of first-line defence
First-line defences are not completely effective. Some pathogens, such as hepatitis A virus and cholera bacteria, can survive passage through the stomach's acidic environment.
Second line of defence
When pathogens breach the first line of defence, the second line responds rapidly to invasion. This response is non-specific, treating all pathogen types identically without distinguishing between different species.
Key terms:
- Second line of defence – Phagocytic cells and antimicrobial proteins that act against any invading microorganism that has penetrated the first line of defence
- Non-specific defences – Innate defences that do not distinguish between pathogen types, giving identical responses upon each encounter. These act quickly but are not always highly effective
Blood clotting
Blood clotting provides a rapid response to wounding. Platelets and blood vessel lining cells release compounds initiating a cascade – a complex chain reaction involving numerous plasma proteins. Clotting serves multiple functions:
- Prevents blood loss
- Blocks pathogen entry
- Provides a protective surface for wound healing
The cascade's multiple steps amplify a small stimulus to produce large quantities of fibrin rapidly, sealing the wound.
The cascade mechanism is an example of signal amplification in biological systems. Each step in the cascade activates multiple molecules of the next enzyme, creating an exponential increase in the response. This allows a small initial stimulus to rapidly produce enough fibrin to seal a wound effectively.
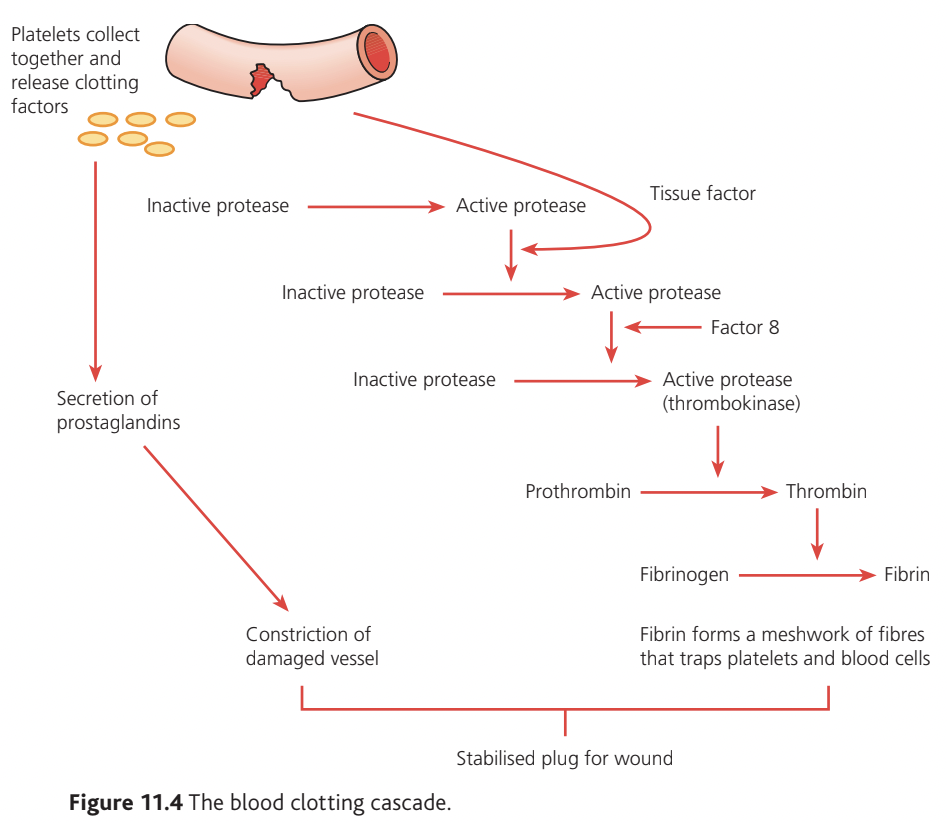
The cascade proceeds as follows:
- Platelets aggregate at injury sites, releasing clotting factors
- Inactive proteases are sequentially activated through tissue factor and Factor 8
- Thrombokinase (active protease) converts prothrombin to thrombin
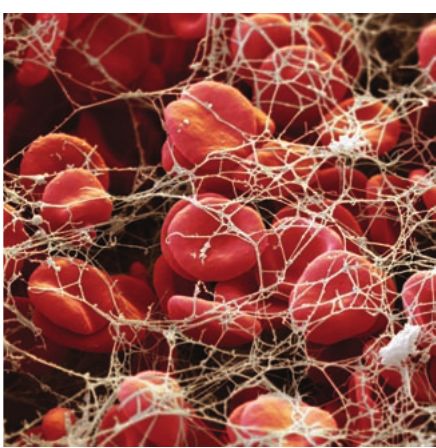
- Thrombin converts fibrinogen to fibrin
- Fibrin forms a meshwork that traps platelets and blood cells
- Prostaglandin secretion causes vessel constriction
- A stabilised plug forms over the wound
Inflammation
Inflammation manifests as redness, swelling, heat, and pain around wounds. These visible features result from coordinated cellular and chemical defence responses recruited from the blood.
Key term: Inflammation – A local response to tissue damage and infection involving chemical signalling molecule release, resulting in increased blood flow and phagocyte movement into infected tissues.
Mast cells throughout the body respond to tissue damage by secreting histamine. This cell-signalling compound stimulates several responses:
- Vasodilation increases capillary blood flow
- Increased capillary permeability allows fluid entry into tissues, causing swelling
- Phagocytes leave blood vessels, entering tissues to engulf foreign material
- Plasma proteins leave the bloodstream
Histamine stimulates cells to secrete cytokines, which promote local and systemic defences. Interleukin 1 (IL-1) and interleukin 6 (IL-6) promote inflammation. Cytokines also stimulate hepatic release of acute phase proteins, some binding to bacterial surfaces and damaged host cells to enhance phagocytosis.
Key term: Cytokines – Small protein molecules functioning as cell-signalling compounds. Many stimulate infection responses including inflammation and immune responses. Interleukins are cytokines.
Systemic Effects of Inflammation
C-reactive protein concentration increases over 1000-fold at infection onset, serving as a useful clinical marker for inflammation. Cytokines produce systemic effects beyond the local site: IL-1 stimulates the brain, causing fever and drowsiness. These symptoms, while uncomfortable, are actually part of the body's defence mechanism—fever inhibits pathogen reproduction and drowsiness promotes rest, allowing energy to be directed toward the immune response.
Wound repair
Wound healing involves overlapping stages:
- New blood vessel formation
- Collagen production
- Granulation tissue formation filling the wound
- New epithelial cell formation through stem cell division and migration
- Wound contraction by contractile cells
- Programmed death of unnecessary cells
Stem cells beneath scabs divide by mitosis to repair wounds. Platelets secrete growth factors attracting and stimulating cell division.
Phagocytes
Phagocytes engulf pathogens and foreign material through phagocytosis. Three main types exist: neutrophils, monocytes/macrophages, and dendritic cells.
Neutrophils circulate in blood and enter tissues during infection. They function as a 'rapid reaction force', responding quickly to infected areas. Neutrophils are short-lived cells that die after destroying bacteria, sometimes accumulating as pus. They constitute - of all white blood cells.
Key term: Neutrophil – A short-lived phagocytic cell produced in bone marrow that circulates in blood. Neutrophils have lobed nuclei and granular cytoplasm.
Monocytes leave blood vessels and enter tissues, differentiating into macrophages ('big eaters'). These long-lived cells process and present antigens to lymphocytes. Some macrophages migrate; others remain stationary in organs (kidneys, lungs, brain, liver) and especially in the spleen and lymph nodes where extensive antigen presentation occurs.
Key terms:
- Monocyte – A larger cell than a neutrophil that circulates in blood and leaves to become a long-lived tissue macrophage
- Macrophage – A large, long-lived phagocytic cell residing in tissues that processes pathogens and presents antigens to T lymphocytes
Dendritic cells possess long processes providing large surface areas for interaction with pathogens and lymphocytes. Found throughout the body, they migrate to lymph nodes after ingesting foreign material.
Key term: Dendritic cell – A large phagocytic cell with lengthy extensions providing large surface area for pathogen and lymphocyte interaction.
Neutrophil numbers increase rapidly during infection. They pour from bone marrow, circulate in blood, then leave through capillary walls into damaged tissues. During lung infections, neutrophils traverse alveolar capillary walls and digest through alveolar lining to reach bacteria. This remarkable ability to migrate through tissues demonstrates the highly coordinated nature of the immune response.
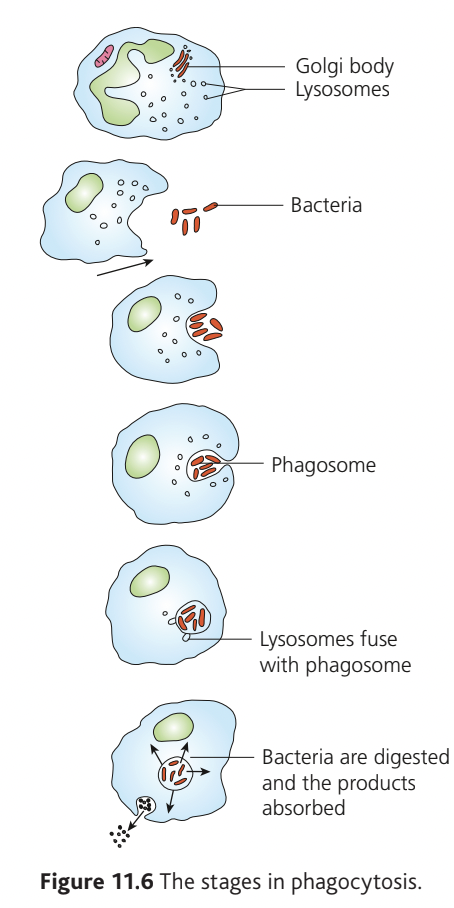
Phagocytosis proceeds through these stages:
- Bacteria approach the cell
- Cell membrane engulfs bacteria
- Phagosome forms around bacteria
- Lysosomes fuse with the phagosome
- Bacteria are digested
- Products are absorbed into the cytoplasm
Third line of defence
Phagocytes alone provide insufficient defence. A system recognising specific invading organisms is required. Lymphocytes and antibodies provide this specific defence system, which identifies different pathogens entering the body.
Key term: Third line of defence – A response to invading pathogens in which lymphocytes and antibodies act against specific pathogens.
Specific defences are highly effective but slower than non-specific defences. Humans are not born with these defences but possess the potential to produce specialised lymphocytes and antibodies for every pathogen strain that exists or may exist in future.
The immune system must be able to recognize an almost infinite variety of potential pathogens. Remarkably, humans possess the genetic capacity to produce specialized lymphocytes and antibodies for virtually any antigen that might exist—even those that have never been encountered before in human history.
The sequence of changes selecting and amplifying specialised lymphocytes is the immune response – an adaptive response to environmental changes (pathogen entry) that enhances survival if that pathogen reinvades.
Key term: Immune response – The sequence of events occurring as the specific immune system responds to a foreign antigen, potentially involving B cell or T cell clonal activation.
Lymphocytes
Lymphocytes are small white blood cells active in tissues rather than blood. They congregate in lymph nodes throughout the body, especially in areas prone to infection (throat, gut, lungs, reproductive system).
Two lymphocyte groups exist:
- B lymphocytes (B cells): Originate from bone marrow stem cells, differentiating into mature cells that spread through the lymphatic system
- T lymphocytes (T cells): Originate in bone marrow but migrate to the thymus gland for maturation before populating the lymphatic system
Key terms:
- B lymphocyte – White blood cell type maturing in bone marrow; responding B cells become plasma cells
- T lymphocyte – White blood cell type maturing in the thymus gland; responding T cells do not produce or release antibodies

During maturation, B cells and T cells acquire cell surface receptors – transmembrane glycoproteins with specifically shaped extracellular regions. Mature B cells have receptors with identical specificity to the antibodies they will secrete. Each B cell type has a differently shaped B cell receptor (BCR) identifying its specificity. Each T cell type has T cell receptors (TCRs) identifying its specificity.
The Diversity of Immune Recognition
This huge variation in BCRs and TCRs enables lymphocyte recognition of surface molecules on invading microorganisms and their products (e.g. toxins from tetanus, cholera, and diphtheria bacteria). Each lymphocyte displays approximately receptors on its surface, all with identical specificity.
An estimated different antibody receptor types can be generated through gene coding sequence rearrangement. This provides sufficient variation to recognise any conceivable antigen type. Although numerous B and T cells exist in the body, only small numbers of each type are present.
Key term: Clone – A group of genetically identical cells. In the immune system, B cell and T cell clones exist, each with unique cell surface receptors complementary to specific antigens.
Among all clones are B cells and T cells with receptors specific to the same antigen, enabling coordinated responses to the same threat. Lymphocytes circulate between blood, lymph, lymph nodes, spleen, and liver, contacting any pathogens, toxins, foreign material, and antigen-presenting macrophages and dendritic cells.
Antigen-presenting cells
Unlike neutrophils that completely destroy engulfed material, macrophages and dendritic cells process pathogens differently. They fragment pathogens and incorporate bacterial and viral surface components within cell surface membrane proteins. These proteins display antigens, presenting them to nearby lymphocytes.
Antigen presentation is crucial for initiating immune responses. However, this capability is not unique to macrophages and dendritic cells; many cell types perform this function using different display proteins. This widespread ability ensures that the immune system can detect infections throughout the body.
B cell activation
B cells respond directly to large molecules with repeated structures, such as bacterial surface polysaccharides. These antigens interact with multiple BCRs on B cell surfaces. This multiple interaction sufficiently activates B cells to divide and differentiate into plasma cells.
Key term: Plasma cell – An activated B cell that produces and releases antibodies during immune responses.
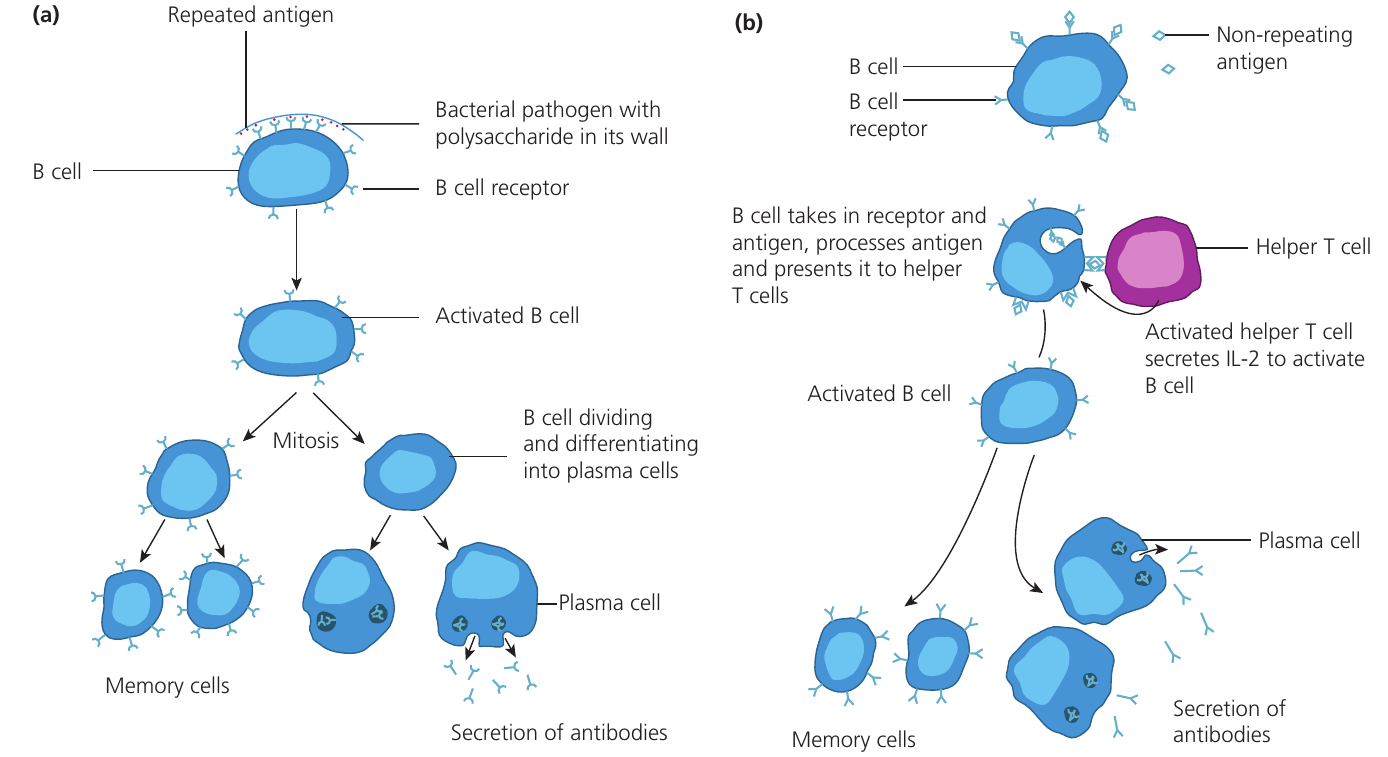
B cells also respond to soluble antigens (e.g. protein molecules) that interact with single BCRs. Antigens within BCRs are internalised by endocytosis, processed, attached to display proteins, and presented on cell surfaces. T helper cells with complementary TCRs are activated and secrete interleukin 2 (IL-2), stimulating B cell division and plasma cell differentiation. This fail-safe mechanism prevents unnecessary antibody release.
During clonal expansion, some activated B cells become plasma cells, synthesising numerous ribosomes and rough endoplasmic reticulum. Antibody genes are transcribed, mRNA translated, and polypeptides assembled into antibody molecules. These molecules are processed in the Golgi apparatus, packaged into vesicles, and exported by exocytosis. Other clone members remain inactive, circulating as long-lived memory cells between blood and lymphatic system.
T cell activation
T helper cells are central to immune responses, responding to macrophage-presented antigens and stimulating both B and T cells.
Key term: T helper cells – T cell type coordinating immune responses by stimulating B cell and T killer cell responses through chemical signals such as interleukins.
Immune responses involving T helper cells proceed through these stages:
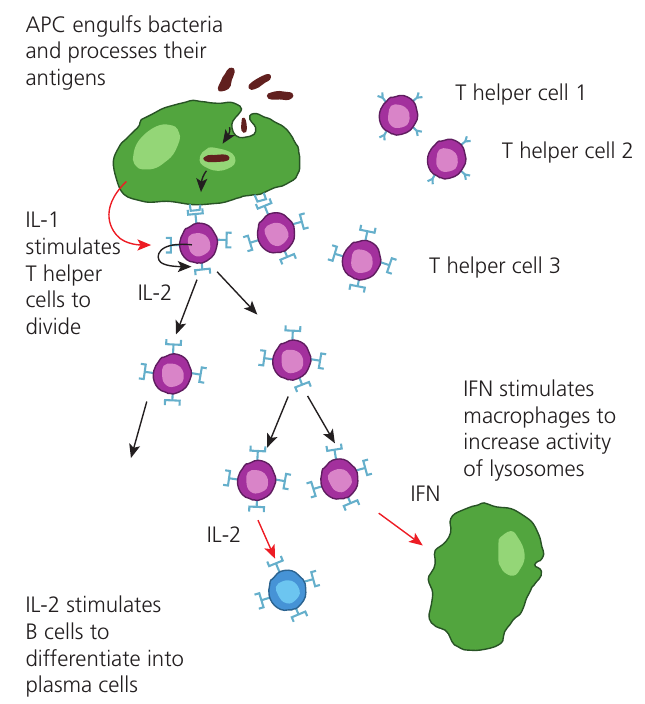
1. Antigen presentation: Antigen-presenting cells (APCs) – macrophages and dendritic cells – in lymph nodes engulf pathogens by endocytosis, fragment them, process surface antigens, and display them in special cell surface membrane proteins
2. Clonal selection: T cells with receptors complementary to presented antigens bind to macrophages. These specific small T cell groups are selected clones. APCs secrete interleukin 1 (IL-1) to activate selected T helper cells
Key term: Clonal selection – The process during immune responses when specific B cell and/or T cell clones interact with APC-displayed antigens.
3. Clonal expansion: Because few T cells can destroy invading pathogens, clone members divide by mitosis to form larger clones. T helper cells release IL-2 to stimulate B cell division and plasma cell differentiation, coordinating different lymphocyte activities plus macrophages and other immune components. IL-2 also self-stimulates T helper cells to increase cytokine production, including interferon (IFN), which stimulates macrophage activity
Key term: Clonal expansion – Mitotic division of small identical B cell and T cell groups during immune responses, generating effector cells (e.g. plasma cells) and memory cells.
4. Antibody production: Stimulated B cells form plasma cells secreting appropriate antibodies
Most antibodies produced upon first antigen presentation are large molecules with ten identical antigen-binding sites. These super-large antibodies effectively agglutinate bacteria, causing them to clump together and making them easier targets for phagocytes.
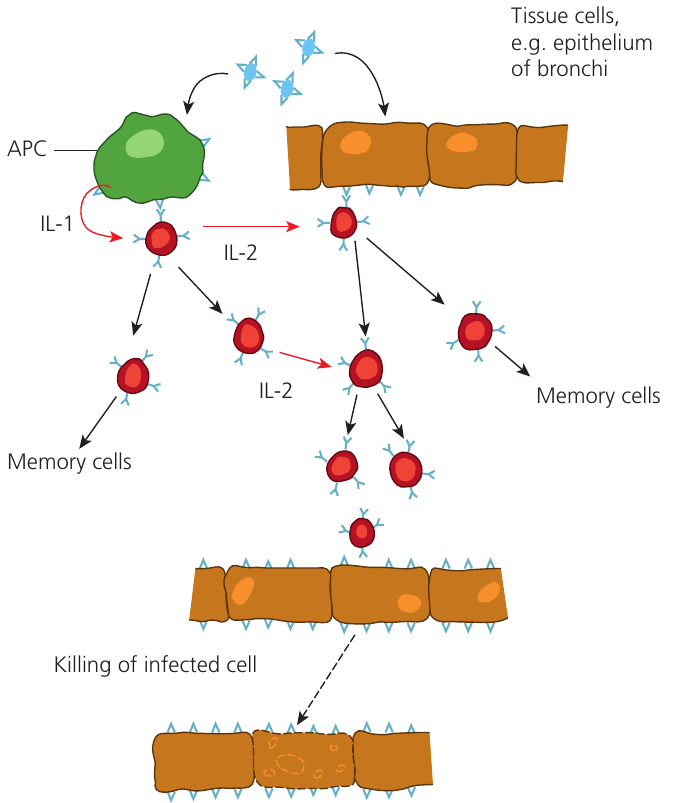
Cells continuously fragment internal proteins and present resulting short peptides within cell surface proteins, displaying their contents to patrolling T killer cells. When T killer cells encounter infected cells expressing foreign antigens specific to their TCRs, they become active only if TCR shape complements the antigen.
Key term: T killer cell – T cell type that kills infected host cells.
Once activated, T killer cells bind to infected cell surfaces and secrete perforins – proteins inserted into infected cell membranes. Perforins form channels allowing toxin entry (hydrogen peroxide, nitric oxide), killing host cells. Though drastic, this is necessary to eliminate intracellular pathogens such as M. tuberculosis and viruses like measles and influenza. Specific T helper cells activate simultaneously, promoting appropriate T killer cell clone expansion by secreting IL-2.
While killing the body's own cells may seem counterproductive, it is essential for destroying intracellular pathogens that cannot be reached by antibodies or phagocytes. Without T killer cells, viruses and bacteria that hide inside cells would be able to reproduce unchecked.
Immune responses require regulation. T regulator cells down-regulate immune responses, shutting them down after pathogen removal and preventing T cell attacks on the body's own cells and tissues.
Key term: T regulator cell – T cell type that stops immune responses and prevents T cell self-attack on body cells and tissues.
Memory cells and long-term immunity
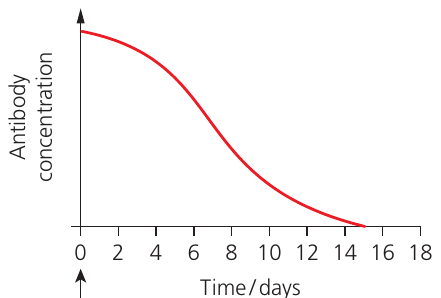
The primary immune response takes approximately - days for antibodies to appear in blood after initial antigen entry. This delay explains illness during first infections (e.g. chickenpox). Eventually, antibodies and activated T killer cells remove the infectious agent, enabling recovery.
Plasma cells are short-lived, and their antibodies are soon degraded. However, upon second antigen entry, the response accelerates significantly. During clonal expansion, B and T cells form memory cells that continue circulating in blood and lymph, patrolling for antigen return.
Primary vs Secondary Immune Response
Upon antigen return, memory cells respond faster because their numbers exceed the original clone before first infection. The secondary immune response occurs much faster than the primary response, rarely producing infection symptoms. Secondary responses may take only days for antibody concentration increases due to memory cell activation. Responses are greater (more antibodies produced) and longer-lasting.
This principle forms the basis of vaccination effectiveness—by exposing the immune system to harmless forms of pathogens, we create memory cells that provide rapid protection if the real pathogen is encountered later.
'Memory' is somewhat misleading – these cells have not 'learned' anything but simply represent an enlarged clone.
Antibodies
Antibodies are plasma proteins called immunoglobulins (Ig). All antibodies have quaternary structure, formed from four or more polypeptides. The simplest antibody form (Ig class G, or IgG) comprises four polypeptides. Other classes contain more than four polypeptides, with the largest having polypeptides.
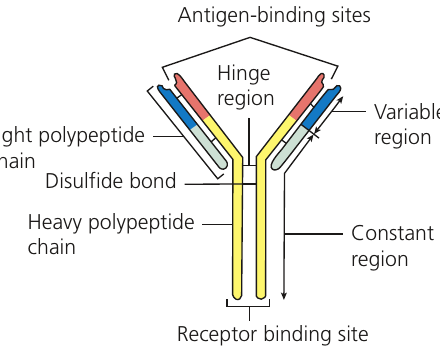
Each IgG molecule consists of two identical long (heavy) polypeptides and two identical short (light) polypeptides. The antibody region binding antigens – the antigen-binding site – is located at the Y-shaped molecule's two upper ends. Polypeptides are held together by disulfide bonds. The hinge region provides flexibility, allowing binding sites to contact variably separated antigens.
The constant region is identical for all antibodies of the same class. All IgG constant regions are identical regardless of variable region specificities. These regions bind to phagocyte surface receptors, helping phagocytes detect antibody-labelled pathogens for phagocytic destruction.
For specific antigen binding, each antibody type has different antigen-binding sites. Amino acids can be arranged in numerous sequences, generating different three-dimensional shapes. Because these binding sites vary, they are called variable regions. These resemble enzyme active sites and cell-signalling molecule receptor binding sites – all have specific shapes complementary to binding agents.
Antibody Specificity
Antibody molecule antigen-binding sites are complementary in shape to their specific antigens. Numerous antibodies with different variable regions are needed to 'fit around' different body-entering antigens. Better antigen-antibody 'fit' produces more efficient immune responses for pathogen identification and destruction. This is similar to the lock-and-key or induced-fit model of enzyme action.
Within each antibody class, antibodies function differently in defence. Some act as:
- Antitoxins: Combine with bacterial toxins (e.g. tetanus, diphtheria) rendering them harmless
- Agglutinins: Bind to identical antigens on multiple pathogens, causing clumping. This hinders spread and facilitates phagocytosis. The largest antibody class (ten antigen-binding sites) is more effective than classes with only two sites
- Opsonins: 'Coat' pathogens to facilitate phagocytosis. Phagocytes have antibody constant region receptors. By attaching to bacteria, these antibodies 'mark' them for phagocytic destruction. Opsonisation is likened to 'sugaring' pills for easier swallowing
Types of immunity
Content considered so far involves active immunity – occurring when antigens enter the body. This may happen naturally through infection or artificially through vaccination. Active immunity always involves immune responses, providing long-term (often lifelong) protection.
Active Immunity
- Natural active immunity: Occurs through infection
- Artificial active immunity: Results from vaccine administration containing one or more antigens
Both forms involve the immune system producing its own antibodies and memory cells, leading to long-lasting protection.
Immunity can also be gained by receiving antibodies from another person – passive immunity. The body gains antibodies from external sources without antigen contact or immune responses. Passive immunity may be natural or artificial.
Passive Immunity
- Natural passive immunity: Occurs when antibodies cross the placenta during pregnancy or through breastfeeding. Breast milk contains abundant IgA antibodies against diseases the mother has experienced
- Artificial passive immunity: Occurs when antibodies are injected to provide instant immunity. People potentially exposed to tetanus, rabies, or diphtheria often receive antitoxin injections as precaution. Each antitoxin neutralises pathogen-released toxins, preventing damage
Passive immunity provides immediate but temporary protection since no memory cells are formed.

Autoimmune diseases
The body sometimes self-attacks using antibodies and T cells targeting its own cells. In the UK, approximately of people have autoimmune diseases.
Autoimmune diseases occur when the immune system attacks self-antigens (usually proteins). Autoreactive T helper cells, T cytotoxic cells, and B cells are involved. Sometimes attacks target one organ; other times the whole body is affected, as in systemic lupus erythematosus (SLE) or lupus.
A common lupus symptom is the butterfly-shaped facial rash. The disease affects multiple organs (heart, lungs, kidneys) and causes joint pain. Lupus symptoms vary between flare-ups, complicating diagnosis. Women are far more susceptible than men.
Rheumatoid arthritis is another long-term destructive process occurring in joints. It begins in finger and hand joints, spreading to shoulders and other joints. Constant pain and muscle spasm occur. Tendons become inflamed, and patients often experience lethargy. (Note: osteoarthritis is not an autoimmune disease.)
Understanding Autoimmune Disease Causes
Autoimmune disease causes are poorly understood and heavily researched. Genetic factors contribute, as susceptibility is inherited. However, environmental factors are also important, evidenced by increased prevalence in developed countries over the last years. People migrating from areas where these diseases are rare (e.g. Japan) to areas where they are common (e.g. USA) have increased disease risk.
This suggests that both genetic predisposition and environmental triggers work together to cause autoimmune conditions.
Key Points to Remember:
-
The body employs three defence lines: physical/chemical barriers preventing pathogen entry (first line), non-specific cellular responses including phagocytosis and inflammation (second line), and specific immune responses involving lymphocytes and antibodies (third line)
-
Non-specific defences (phagocytes, blood clotting, inflammation) act rapidly against any pathogen type without distinguishing between species, whilst specific defences (lymphocytes producing antibodies and cell-mediated responses) target particular antigens but take longer to develop
-
Memory cells formed during primary immune responses enable faster, stronger secondary responses upon pathogen re-entry, providing long-term immunity that is the basis for vaccination effectiveness
-
Antibodies possess quaternary structure with variable regions (antigen-binding sites) complementary to specific antigens and constant regions binding phagocyte receptors, enabling them to function as antitoxins, agglutinins, or opsonins
-
Active immunity (natural through infection or artificial through vaccination) involves immune responses creating long-term protection, whilst passive immunity (natural from mother or artificial through antibody injection) provides temporary protection without immune responses