Human Immune System: Further Exploration (HSC SSCE Biology): Revision Notes
Human Immune System: Further Exploration
The immune response after primary exposure to bacteria
Bacteria are among the most common causes of human infections. When your body encounters bacteria for the first time, it launches a comprehensive immune response involving both innate and adaptive immunity systems working together. Understanding how these systems respond helps explain why different bacterial infections require different treatments and why some infections are more serious than others.
Innate immune responses
The innate immune system provides your body's first line of defence against bacterial invaders. This response is rapid and non-specific, meaning it attacks any bacterial threat in similar ways. Several key mechanisms work together to combat bacterial infections.
Complement protein action
Complement proteins are crucial components of the innate immune system that directly attack bacterial cells. These proteins form structures called membrane attack complexes that literally puncture holes in bacterial cell walls and membranes. When these holes form, extracellular fluid rushes into the bacterial cell, causing it to swell and eventually burst through a process called osmotic lysis. This is similar to popping a balloon by overfilling it with water.
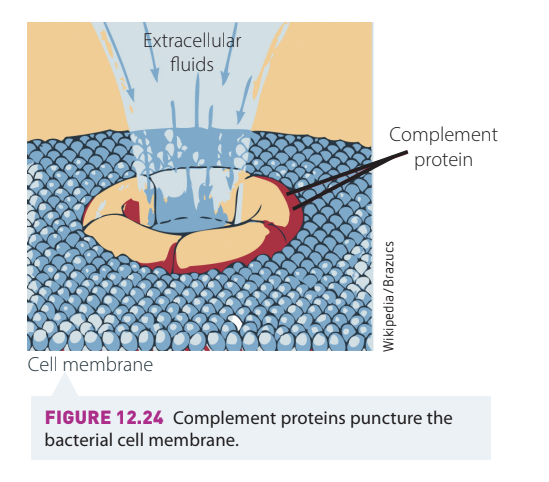
The complement system works like a molecular drill, creating pores that allow water to flood into bacterial cells. The resulting osmotic pressure causes the bacteria to burst, effectively eliminating the threat before it can multiply.
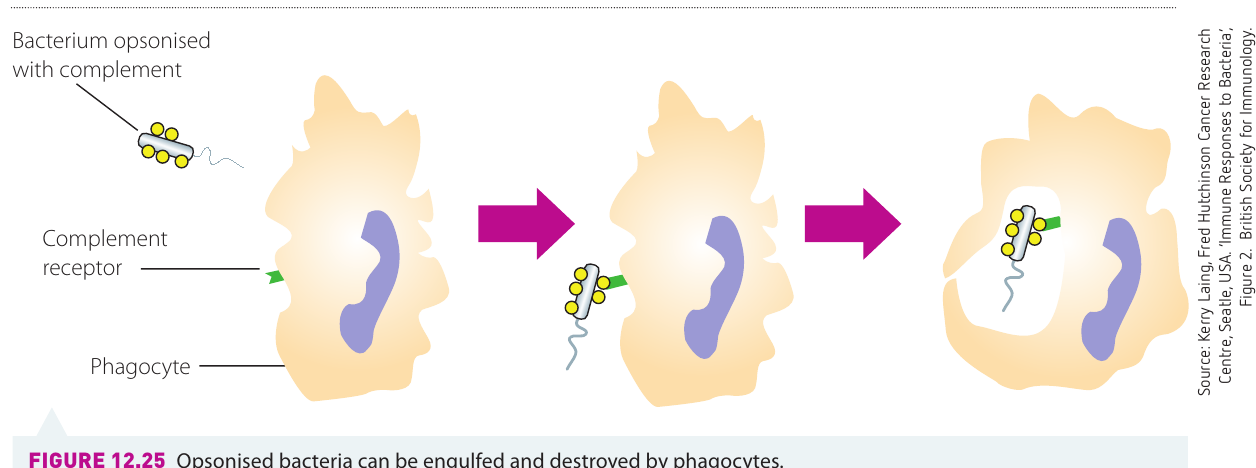
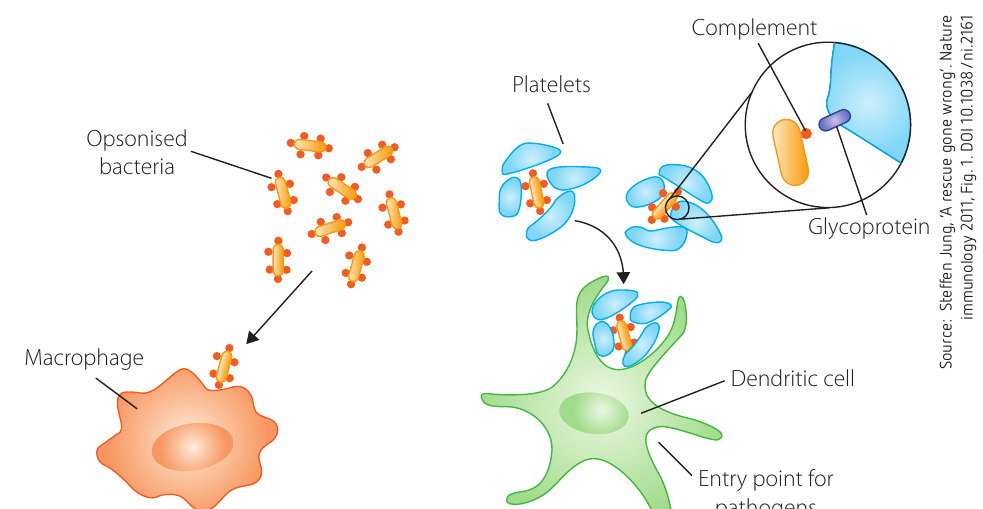
Opsonisation and phagocytosis
Opsonisation is a process where bacteria become coated with special molecules (antibodies and complement proteins) that make them easier for immune cells to recognise and destroy. Think of opsonisation as "tagging" the bacteria for destruction. Once bacteria are opsonised, phagocytes (cells that engulf and destroy pathogens) can easily identify and consume them through phagocytosis.
White blood cell responses
Different types of white blood cells respond in characteristic ways to bacterial infections. Neutrophils are particularly important during bacterial infections and show increased activity. When you have a bacterial infection, your bone marrow increases neutrophil production, causing neutrophil levels in your peripheral blood to rise. This increase is especially common with Gram-positive bacterial infections. However, in severe infections, neutrophil numbers may actually decrease (neutropaenia) because the demand for these cells exceeds the bone marrow's ability to produce them.
In severe bacterial infections, neutrophil numbers may paradoxically decrease despite increased demand. This neutropaenia occurs when the body's demand for these cells exceeds the bone marrow's production capacity, indicating a potentially life-threatening situation requiring immediate medical attention.
Monocytes (another type of white blood cell) may also increase in number, particularly as the infection begins to resolve. This increase is called monocytosis and indicates that your body is working to clear the infection.
Adaptive immune responses
The adaptive immune system provides a more targeted response to bacterial infections. Unlike the innate system, adaptive immunity can distinguish between different types of bacteria and "remembers" previous infections. The specific adaptive response depends on whether the bacteria live inside cells (intracellular) or outside cells (extracellular).
Intracellular bacteria
Some bacteria, such as Salmonella, survive and multiply inside host cells where complement proteins and antibodies cannot reach them. To combat these bacteria, your body uses cell-mediated immunity. Infected macrophages display bacterial proteins on their surface using special molecules called MHCII receptors. Helper T cells recognise these displayed proteins and release interferon, a signalling molecule that stimulates the macrophage to destroy the bacteria inside it. This represents an excellent example of innate and adaptive systems cooperating to solve the same problem.
Innate-Adaptive Cooperation:
The fight against intracellular bacteria demonstrates how innate and adaptive immunity work as a team. Macrophages (innate) cannot destroy intracellular bacteria alone, but when helper T cells (adaptive) release interferon, they activate the macrophages to complete the job. This partnership is essential for clearing infections that would otherwise be impossible to eliminate.
Extracellular bacteria
Extracellular bacterial infections, such as those caused by Staphylococcus aureus, are the most common type. Protection against these bacteria relies on natural barriers (like skin), innate immune responses, and antibody production by the adaptive immune system.
The table below summarises how different parts of the immune system respond to bacterial infections:
| Immune Component | Response Mechanism |
|---|---|
| Natural barriers | Skin, mucous membranes, sebum, urine, gastric acid |
| Innate immunity | Complement proteins, phagocytes (natural killer cells, neutrophils, macrophages) |
| Adaptive immunity | Antibody production by plasma cells, cytokine production by T cells, memory B cell formation |
The role of gut microbiome
Your gut contains trillions of beneficial bacteria collectively called the microbiome. These bacteria play a major protective role in regulating immune responses and preventing disease. From birth onwards, your gut becomes colonised by these helpful microbes. Research shows that symbiotic bacteria in the human gut help prevent inflammatory diseases and provide extensive molecular interactions with your immune system.
Colonisation resistance
One crucial function of the gut microbiome is colonisation resistance—the ability to prevent harmful pathogens from establishing infections. The microbiome achieves this through several mechanisms:
- Competing with pathogens for space and nutrients
- Producing inhibitory molecules that block pathogen growth
- Communicating with pathogens through quorum sensing (bacterial cell-to-cell communication)
Quorum sensing allows beneficial gut bacteria to detect and respond to pathogenic bacteria. For example, Ruminococcus obeum, a beneficial gut microbe, can sense signals from pathogens like Vibrio cholera and produce molecules that prevent the pathogen from colonising the gut.
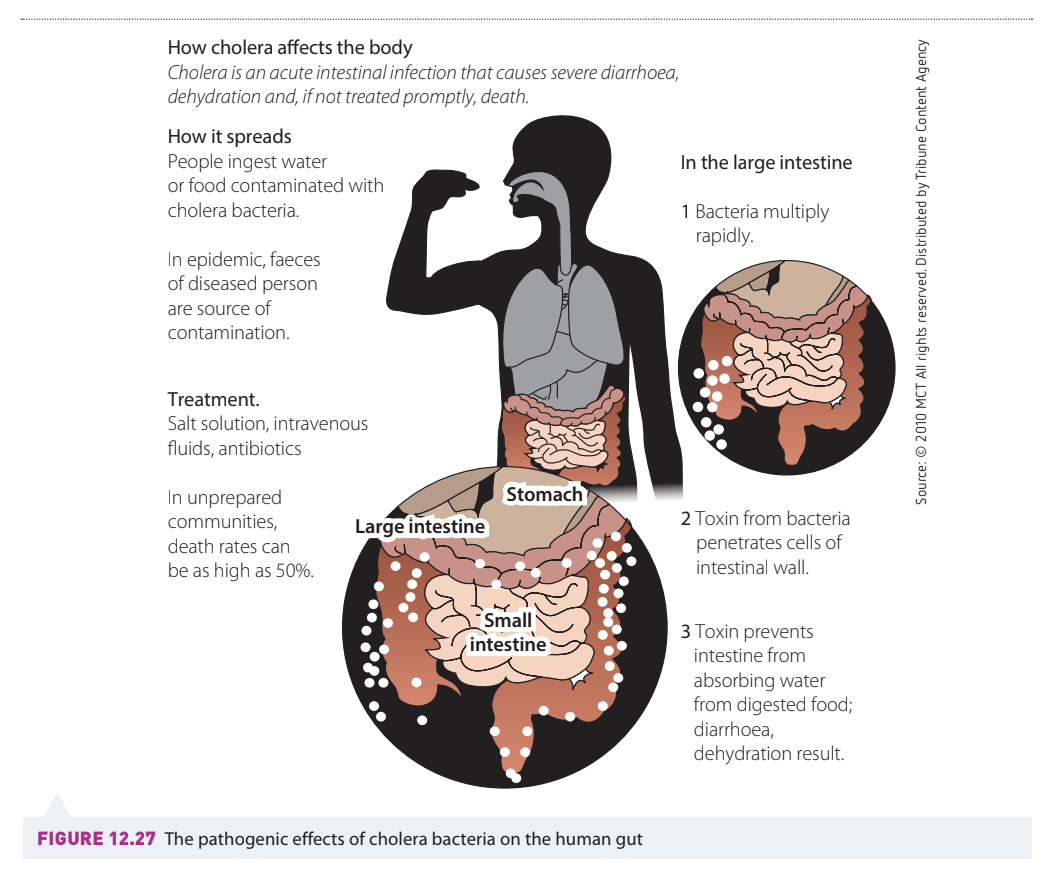
Case study: immune responses to Vibrio cholera (cholera)
Cholera affects millions of people worldwide, particularly in developing countries. The infection causes severe, profuse diarrhoea and vomiting. Without prompt treatment, death can occur from severe dehydration and shock due to massive fluid loss. Understanding how the immune system responds to cholera helps explain both why the disease is so dangerous and how immunity develops.
The pathogen
The bacterium that causes cholera is Vibrio cholera, a curved or comma-shaped (vibrio) Gram-negative rod. This bacterium produces toxins that dramatically affect the human digestive system.
Innate immune response to cholera
When Vibrio cholera enters the gut, the innate immune system responds rapidly:
- Cytokines such as interleukin are produced to signal immune cells
- Neutrophils migrate into the gut lining to combat the infection
- Antibacterial peptides called defensins are produced—these either kill bacteria directly or alter host gene expression to produce more cytokines and induce inflammation
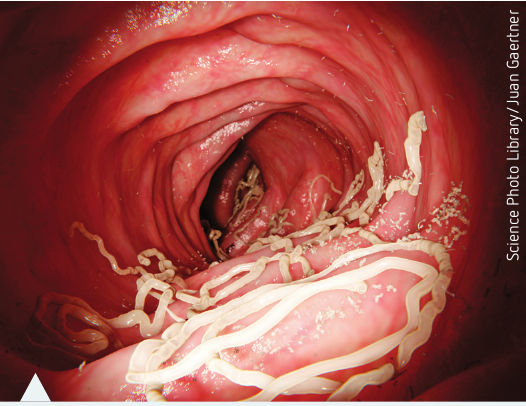
Adaptive immune response to cholera
The adaptive response to cholera develops more slowly but provides longer-lasting protection:
- IgA antibodies are secreted by the gut lining to protect against bacterial colonisation
- After approximately one week, circulating B lymphocytes specific to V. cholera antigens increase
- Serum antibody levels peak at weeks after initial infection
- Antibody levels gradually decrease after about one year
- Memory B cells form and provide a secondary response if the person encounters the bacterium again
The graph shows how different components of the adaptive immune response develop over time, with antibody-secreting cells appearing first, followed by peak antibody levels, and finally long-lasting memory B cell responses.
How cholera evades the immune system
Vibrio cholera has developed clever strategies to evade immune defences. The bacterium attaches small amino acids to large endotoxin molecules on its outer surface. These modifications change the bacterial membrane's electrical charge from negative to neutral.
This charge change is critical because the molecules your body produces to fight bacteria (cationic antimicrobial peptides, or CAMPs) carry positive charges. Normally, CAMPs bind to negatively charged bacterial surfaces, create pores in the membrane, and kill the bacteria. However, when V. cholera creates a neutrally charged surface, CAMPs cannot bind and the bacteria survive.
Cholera's Survival Strategy:
V. cholera cleverly evades immune destruction by changing its surface charge from negative to neutral. This prevents positively charged antimicrobial peptides (CAMPs) from binding to the bacterial surface. With this protection, V. cholera can invade the gut wall and cause the dramatic symptoms of cholera. Although the adaptive immune response eventually activates, it often doesn't reach protective levels quickly enough. The severe diarrhoea and vomiting can kill the person before immunity fully develops.
During this process, the body's beneficial microbiota are also outcompeted by the pathogen.
Future treatment possibilities
Researchers are working to develop drugs that could disable the amino acids V. cholera uses for protection. If successful, CAMPs could function normally and the innate immune system would prevail, potentially saving lives.
The immune response after primary exposure to fungi
Humans constantly encounter fungi through eating, breathing, and skin injuries. Despite this frequent exposure, most fungi cause no disease in healthy people. Superficial fungal infections of the skin (caused by dermatophytes) are the most common type of fungal infection. Understanding how the immune system responds to fungi helps explain why some people develop fungal infections while others remain healthy.
Innate immune responses
The innate immune system plays a major role in defending against fungal pathogens. Physical barriers such as skin and mucous membranes provide the first line of defence, preventing most fungi from entering the body.
When fungi do breach these barriers, phagocytes become the primary defenders. Dendritic cells, neutrophils, and macrophages all contain pattern recognition receptors (PRRs) on their surface. These receptors recognise and bind to characteristic fungal structures. Once bound, the phagocytes can engulf and destroy the fungal cells.
During fungal infections, neutrophil numbers in the peripheral blood commonly increase, providing additional defensive capacity.
Adaptive immune responses
Scientists still have much to learn about adaptive immune responses to fungi. Both cell-mediated immunity and humoral immunity (antibody production) contribute to antifungal defence, though their exact roles remain incompletely understood.
Key adaptive responses include:
- Phagocytosis initiates the response and alerts other immune cells through cytokine production, inducing inflammatory responses
- Dendritic cells transport ingested fungi to lymph nodes, where helper T cells and memory T cells are recruited and activated
- Helper T cells produce interleukin-17, which further stimulates neutrophils and macrophages
- Interleukin-17 is critical for antifungal immunity because it promotes inflammation that helps clear the infection
Critical Role of Interleukin-17:
Interleukin-17 is absolutely essential for antifungal immunity. This cytokine promotes the inflammatory response necessary to clear fungal infections. Without adequate interleukin-17 production, fungal infections can become chronic and difficult to eliminate.
Case study: immune responses to Trichophyton rubrum (tinea)
Dermatophyte infections rank among the world's most common fungal infections. They primarily affect body skin (tinea corporis), feet (tinea pedis or "athlete's foot"), and nails (tinea unguium). Understanding tinea helps illustrate how fungi can sometimes evade immune responses.
The infection
Tinea pedis causes scaling, redness, and itching of the feet and toes. It is particularly common in South-East Asia, Africa, and parts of Australia, likely due to less frequent use of enclosed footwear in these regions.
How the fungus evades immunity
Evidence suggests that T. rubrum can sometimes evade initial innate immune responses. When this happens, adaptive T cell responses never activate because they depend on signals from the innate system. Both innate and adaptive responses are necessary to clear the infection completely.
The Critical Innate-Adaptive Link:
If innate immune responses fail to activate, adaptive responses never begin. This dependency creates a vulnerability that T. rubrum exploits to establish chronic infections. Both systems must work together—failure of the innate system means failure of the entire immune response.
In tissues infected by T. rubrum, several things occur:
- Enzymes called keratinases break down the skin barrier, allowing deeper infection
- Molecules in the fungal cell wall called mannans inhibit immune responses and reduce replacement of superficial skin cells
- Hypersensitivity responses (either immediate or delayed) may develop
Immune system responses
Despite the fungus's evasion strategies, the immune system mounts several responses:
- Keratinocytes (skin cells) express toll-like receptors (TLRs) and produce defensins as a first-line response
- Dendritic cells regulate the overall response—they suppress fungal growth and stimulate cytotoxic T cell production, combining innate and adaptive (cell-mediated) immunity
- Pattern recognition receptors recognise pathogen-associated molecular patterns (PAMPs), allowing phagocytes to express mannose receptors that recognise mannans in the fungal cell wall
- Cytokines are released and phagocytosis of fungal cells occurs
- Cytotoxic T cells proliferate to kill infected cells
Chronic infections
Approximately of patients develop chronic tinea infections, probably due to defective cell-mediated responses. In these patients, cytotoxic T cell responses are depressed. Some fungi can evade mannose receptors on epithelial cell membranes, avoiding recognition. When this happens, no cytokine is released, phagocytosis is not induced, and T cells are inhibited.
Blood tests may show increased neutrophils (neutrophilia) and monocytes (monocytosis). This case illustrates the critical importance of interaction between innate and adaptive immune systems. Without initiation of innate responses, adaptive responses do not activate and infection continues unchecked.
The immune response after primary exposure to viruses
Viruses present unique challenges to the immune system because they must invade host cells to replicate. Once a virus enters a cell, the immune system cannot directly access the virus itself. Instead, infected cells display pieces of viral protein on their surface using MHC class I molecules, essentially "showing" the immune system that they are infected.
Cell-mediated immunity against viruses
The adaptive immune system uses cytotoxic T cells to recognise and destroy virally infected cells. Only T cells with specific receptors for that particular virus become activated—this specificity ensures that healthy cells are not harmed. Once activated, cytotoxic T cells release factors that kill the infected cell, preventing the virus from spreading.
Viral evasion and natural killer cells
Some viruses can prevent MHC class I molecules from reaching the cell surface, hiding the viral infection from T cells. However, the innate immune system has evolved a counter-strategy. Natural killer (NK) cells detect cells with fewer MHC class I receptors than normal and kill them, treating them as potentially infected.
Cellular Surveillance Strategy:
The immune system uses a clever "check and balance" approach: T cells monitor cells displaying viral proteins on MHC class I, while NK cells monitor cells with reduced MHC class I expression. Between these two mechanisms, viruses have difficulty hiding—either they display viral proteins and get detected by T cells, or they reduce MHC class I and get detected by NK cells.
How cytotoxic cells kill infected cells
Cytotoxic cells release several molecules to destroy infected cells:
- Perforin creates pores in the cell membrane
- Granzymes enter through these pores and trigger programmed cell death (apoptosis)
- Cytokines (such as interferon) prevent viral replication inside infected cells
- Interferon also signals neighbouring cells to increase MHC class I molecules on their surface, making them easier for T cells to monitor
Humoral immunity against viruses
Antibodies produced by B lymphocytes can fight viruses before they infect cells. When antibodies coat a virus, the virus can no longer infect cells. Antibody-coated viruses also become targets for phagocytes. Additionally, antibodies activate the complement system, and complement proteins bind to and damage the viral envelope.
Blood count changes in viral infections
Full blood counts can show unpredictable changes during viral infections. The total white cell count may decrease (leukopaenia) because viruses can suppress bone marrow production of white cells. Sometimes lymphocytes and monocytes increase while neutrophils decrease more dramatically, resulting in an overall reduction in white cells.
Case study: immune responses to Dengue fever virus
Dengue fever threatens millions of people worldwide, particularly in tropical countries. The Aedes aegypti mosquito transmits the virus. Understanding Dengue helps illustrate how some viruses specifically attack the immune system itself.
Disease symptoms
Dengue fever typically causes:
- Fever and headaches
- Skin rash and vomiting
- Joint and muscle pain
- Pain behind the eyes (retro-orbital pain)—a characteristic feature
The disease usually resolves after weeks. However, in fatal cases, death typically results from haemorrhage due to severe platelet deficiency.
How Dengue attacks the immune system
The Dengue virus demonstrates remarkable cunning by infecting immune system cells themselves. It specifically targets macrophages and dendritic cells—key components of the innate immune system. Once the innate immune system is compromised, the virus enters the bloodstream and spreads throughout the body, where mosquitoes can acquire it during blood meals and transmit it to new hosts.
Dengue's Devastating Strategy:
Dengue virus targets the very cells meant to fight it—macrophages and dendritic cells. By compromising these key innate immune cells, the virus prevents the normal activation of adaptive immunity. This represents one of the most sophisticated viral evasion strategies known, essentially disabling the alarm system before it can alert the rest of the immune response.
Normal viral response versus Dengue
Normally, dendritic cells recognise viral PAMPs and release interferons. Interferons activate the adaptive immune system, leading to both T and B cell responses. However, Dengue disrupts this process.
In some people infected with Dengue virus:
- Certain types of interferons (type I IFN) are not produced by dendritic cells
- Dendritic cells cannot signal helper T cells to activate
- Any type I IFN that is released has its signalling blocked by the virus
This represents another example of the intricate cooperation required between innate and adaptive responses. The poor innate and adaptive immune responses observed in Dengue patients result from this disruption.
Additional evasion strategies
Dengue virus can form intracellular membrane pockets or vesicles where it hides and replicates. These hiding spots prevent the host cell's pattern recognition receptors from detecting viral PAMPs.
Immunity and complications
During primary infection, the body produces antibodies against the specific virus strain. Some evidence suggests these antibodies can cross-react with other Dengue virus serotypes (different variants), but only when antibody concentrations are high. This cross-protection fades quickly.
People may maintain type-specific antibodies from a Dengue infection for decades. Both memory B cells and long-lived plasma cells develop after infection.
Vaccine Development Challenges:
In some patients, T cells react very quickly upon re-infection and may actually worsen symptoms. This phenomenon raises significant concerns for vaccine development, as vaccines must avoid triggering this enhanced response. Creating a safe and effective Dengue vaccine requires careful balance to stimulate protective immunity without causing immunopathology.
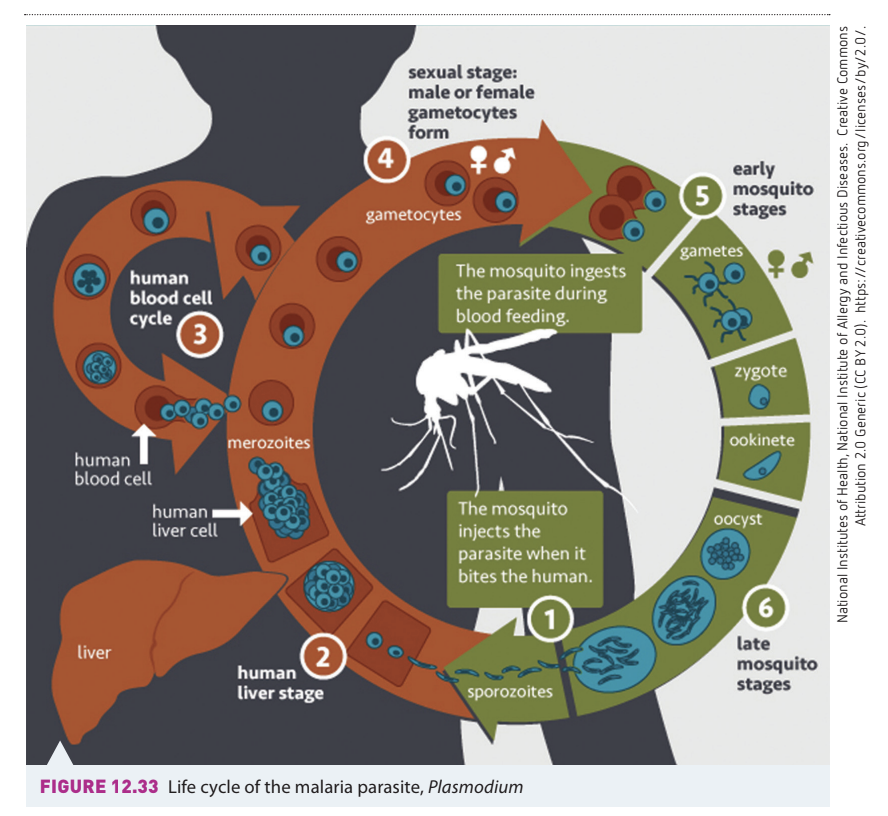
The immune response after primary exposure to protozoa
Protozoa are single-celled organisms (protists) that often display complex, multi-stage life cycles. These complicated life cycles make launching an effective immune response extremely difficult. The malaria parasite Plasmodium provides an excellent example—it cycles between mosquito and human hosts, taking different forms at each stage.
Challenges in fighting protozoal infections
Protozoa typically cause chronic (long-lasting) infections because:
- Innate immune defences are often ineffective against them
- The parasites have evolved numerous mechanisms to resist adaptive immunity
- Different life stages present different antigens to the immune system
Immune responses to protozoa
Protozoa activate different immune responses compared to bacteria, viruses, and fungi.
Blood count changes
Full blood counts typically show eosinophilia (increased eosinophil numbers) due to accelerated bone marrow production. Eosinophils are white blood cells particularly associated with parasitic infections.
Phagocytosis limitations
Although macrophages can phagocytose protozoa, many parasites resist being killed after phagocytosis. Some protozoa can even replicate inside macrophages, turning a defensive mechanism to their advantage.
Parasites Turn Defence Into Advantage:
Some protozoa not only survive phagocytosis but actually replicate inside macrophages—the very cells meant to destroy them. This represents a complete subversion of immune defence, transforming protective mechanisms into safe havens for parasite multiplication.
Escape and evasion mechanisms
Protozoa possess sophisticated strategies for avoiding immune destruction, even in people with healthy immune systems. These escape mechanisms include:
Antigenic masking
The parasite covers itself with host antigens (proteins from the host), essentially disguising itself as part of the host's body. This makes immune recognition extremely difficult.
Blocking of serum factors
The parasite acquires a coating of antigen-antibody complexes or non-cytotoxic antibodies. This coating physically blocks specific antibodies or lymphocytes from binding to the parasite's surface antigens through steric interference (spatial arrangement of atoms preventing binding).
Intracellular location
Living inside host cells protects parasites from direct effects of immune responses. This strategy also delays immune detection by concealing parasite antigens from immune surveillance.
Antigenic variation
The parasite changes its surface antigens during infection. Parasites carrying new antigens escape immune responses directed against original antigens, essentially staying one step ahead of the immune system.
Immunosuppression of the host
Some parasites actively suppress immune function. For example, Plasmodium falciparum (which causes malaria) inhibits maturation of dendritic cells and monocytes in infected red blood cells. This reduced immune response may delay detection of new antigenic variants and reduce the immune system's ability to inhibit parasite growth or kill the parasites.
Case study: immune responses to Plasmodium spp. in malaria infections
People exposed to the malaria parasite Plasmodium falciparum can develop naturally acquired immunity, though exactly how this works remains unclear. Many people in malaria-endemic areas carry large parasite populations in their blood but experience minimal symptoms. These infection levels would be fatal to newly exposed individuals.
Challenges in developing immunity
Many surface proteins of malarial parasites show great antigenic diversity. A host would need an enormous repertoire of antibodies to recognise every possible variation. This diversity makes vaccine development particularly challenging.
Innate immune responses to malaria
Several innate mechanisms provide some protection:
Genetic protection
Some individuals possess inherent protection due to genetic variations affecting haemoglobin or red blood cell structure. Examples include:
- Sickle cell anaemia
- Some thalassaemias
- Duffy-negative red blood cells
These genetic variations make it harder for the parasite to infect red blood cells.
Genetic Trade-offs:
Certain genetic conditions like sickle cell anaemia, while potentially harmful in themselves, provide protection against malaria. This creates an interesting evolutionary trade-off where carrying one copy of the sickle cell gene offers survival advantage in malaria-endemic regions without causing severe disease.
Natural killer cell response
Natural killer (NK) cell numbers increase during infection. NK cells cause lysis (rupture) of parasite-infected red blood cells. They also produce interferon, leading to macrophage activation. NK cells produce chemokines that activate phagocytes and help limit the liver stage of the parasite life cycle.
Adaptive immune responses to malaria
The adaptive system contributes several responses:
Antibody production
Plasma cells produce antibodies, especially IgM and IgG, which can:
- Inhibit merozoite (a parasitic life stage) invasion of red blood cells
- Enhance elimination of infected red blood cells in the spleen
T cell responses
Both helper T cells and cytotoxic T cells contribute to parasite control through various mechanisms.
Stages of acquired immunity
Repeated infections lead to progressively stronger immunity:
- Anti-parasite immunity prevents parasites from entering the blood
- Anti-disease immunity means no clinical symptoms appear despite persistent infection
- Premonition provides protection from new infections due to a low-grade ongoing blood infection with malaria parasites
Opsonisation effects
Opsonisation (coating with antibodies) leads to:
- Increased susceptibility to phagocytosis
- Destruction by cytotoxic T cells
- Parasite inhibition by neutrophils and macrophages
Limitations of acquired immunity
Acquired immunity to malaria does not last indefinitely. If a person leaves an endemic area for an extended period, they become vulnerable to infection again upon return.
Immunity Requires Continued Exposure:
Malaria immunity is not permanent—it requires ongoing low-level exposure to maintain. People who leave endemic areas and return years later become susceptible again, losing the protection they had developed. This has important implications for travelers and migrants.
The immune response after primary exposure to macroparasites
Parasitic worms (helminths) are diverse, antigenically complex organisms that infest millions of people worldwide annually. Infestation by parasitic worms is called helminthiasis. Most infested people experience few signs of infection, but some suffer life-threatening consequences. This remains primarily a problem in developing countries.
Pathogen factors
Macroparasites present unique challenges that differ from other pathogens:
Life cycle complexity
- Many parasitic worms have multiple distinct life stages
- Many worms infest several different hosts as they develop
- Parasites change dramatically before transmission to the next host
- Each life stage may present different antigens to the immune system
Chronic infestations
Prolonged infestations can lead to pathological (disease-causing) changes in host tissues. These changes may persist even after the parasite is eliminated.
Immune evasion
Parasites can modify their surface structure to avoid recognition by the host immune system. This antigenic variation makes developing lasting immunity difficult.
Molecular mimicry
Molecular cross-talk occurs between helminths and the mammalian immune system. The parasites use similar immune signalling molecules to those of the host, potentially confusing immune responses. Schistosomiasis (caused by blood flukes) exemplifies this phenomenon.
Molecular Mimicry Strategy:
Helminths produce molecules that closely resemble the host's own immune signaling molecules. This molecular mimicry can confuse the immune system, making it difficult to distinguish parasite from self. It's like a burglar wearing a security guard uniform to avoid detection.
Host immune responses
Despite the challenges, the immune system mounts predictable responses to helminth infections.
Blood count changes
Full blood counts typically show eosinophilia in response to accelerated bone marrow production of eosinophils. This is one of the most characteristic signs of parasitic worm infection.
Cytokine responses
Th2 cytokines, particularly interleukins, increase during helminth infections. These cytokines help coordinate the immune response to large parasites.
Immune response modulation
The initial T cell reaction is strong but dampens as the infestation becomes chronic. This modulation actually benefits the host by preventing excessive inflammation that could cause tissue damage.
Memory and ongoing protection
An interesting phenomenon occurs with helminth infections: memory cells protect the host from new infections while the original infestation continues. This could work in two ways:
- Adult parasites may successfully evade the immune system
- The primary infestation may alter the host's anatomy or physiology to prevent additional infestations
IgE and resistance
Antiparasite IgE antibody levels correlate with resistance to new infestations. Higher IgE levels generally mean better protection against additional parasites.
Genetic factors
Some families possess Th2 response genes that help confer resistance to helminths. These genes are closely linked with the ability to expel parasites from the body.
Eosinophil function
Eosinophils can kill helminths that have been opsonised (coated with antibodies). This represents cooperation between innate cells (eosinophils) and adaptive immunity (antibodies).
Innate-Adaptive Cooperation in Action:
The destruction of helminths by eosinophils perfectly demonstrates innate-adaptive cooperation. Adaptive immunity provides the antibodies that coat the parasites (opsonisation), while innate eosinophils perform the actual killing. Neither system could eliminate these large parasites alone—teamwork is essential.
Changes in the blood during infectious disease
As part of diagnostic procedures, doctors often request a full blood count (also called complete blood count) when they suspect a patient has an infectious disease. This simple blood test provides valuable information about how the immune system is responding to infection. Understanding what these tests reveal helps doctors make treatment decisions.
What a full blood count reveals
A full blood count determines:
- Absolute numbers of white and red blood cells
- Ratios of different cell types
- Cell features such as sizes, shapes, and structures within the nucleus or cytoplasm (inclusion bodies)
While this test does not always provide a definitive diagnosis or identify the specific pathogen, it can:
- Alert doctors to how the immune system is responding
- Indicate how long the infection has been present
- Show whether the infection is overwhelming the body's defences
- Reveal whether the immune system is mounting an appropriate response
Different types of pathogens generally create characteristic patterns of white and red blood cell changes, making the test a useful diagnostic tool.
Understanding white cell dynamics
The number of white cells circulating in peripheral blood reflects a balance between their use (in responding to infections) and their production rate by bone marrow. Any process affecting either use or production will shift this dynamic equilibrium, resulting in increases or decreases in specific white cell types.
Terminology for blood count changes
Medical terminology uses specific suffixes to describe changes in white cell numbers:
Understanding Medical Terminology:
Increases:
- The suffix "-philia" indicates an increase in total count (e.g., neutrophilia means increased neutrophils)
- The suffix "-cytosis" indicates increased production for some cells (e.g., monocytosis means increased monocyte production)
Decreases:
- The suffix "-paenia" indicates lower than normal numbers (e.g., neutropaenia means decreased neutrophils)
Learning these suffixes helps you interpret blood count results and understand medical reports.
Interpreting a full blood count
A typical pathology report contains multiple components, each providing specific information.
Key components include:
| Component | What it measures | Significance |
|---|---|---|
| White blood cell count | Total number of white cells | Overall immune response level |
| Red blood cell count | Total number of red cells | Oxygen-carrying capacity |
| Haemoglobin | Oxygen-carrying protein | Anaemia indicator |
| Platelet count | Blood clotting cells | Bleeding/clotting ability |
| Differential count | Percentages of each white cell type | Specific immune response pattern |
The differential count breaks down white cells into specific types:
- Neutrophils
- Lymphocytes
- Monocytes
- Eosinophils
- Basophils
Each type increases or decreases in characteristic patterns depending on the infection type.
Patterns associated with different infections
Different pathogens create distinctive blood count patterns:
Bacterial infections typically show:
- Neutrophilia (increased neutrophils)
- Sometimes neutropaenia in severe cases (demand exceeds supply)
- Monocytosis during resolution phase
Viral infections may show:
- Leukopaenia (reduced total white cells)
- Decreased neutrophils
- Increased lymphocytes and monocytes
- The overall decrease reflects bone marrow suppression by the virus
Fungal infections typically show:
- Neutrophilia
- Monocytosis
Protozoal infections usually show:
- Eosinophilia (increased eosinophils)
Parasitic worm infections characteristically show:
- Marked eosinophilia
- This is one of the most reliable indicators of helminth infection
Worked Example: Interpreting a Blood Count
A patient presents with fever and fatigue. Their blood count shows:
- Total white cell count: Low (leukopaenia)
- Neutrophils: Decreased
- Lymphocytes: Increased
- Monocytes: Increased
Analysis: The pattern of leukopaenia with decreased neutrophils but increased lymphocytes and monocytes strongly suggests a viral infection. The virus has suppressed bone marrow production of neutrophils while the body increases lymphocytes to fight the viral pathogen.
Clinical Action: The doctor would avoid prescribing antibiotics (ineffective against viruses) and focus on supportive care, monitoring for complications.
Clinical significance
The full blood count serves as an important diagnostic and monitoring tool. By examining patterns of cell changes, doctors can:
- Distinguish between different types of infections
- Assess infection severity
- Monitor treatment effectiveness
- Detect complications
- Make informed decisions about antibiotic or antiviral therapy
Understanding these blood changes helps explain why your doctor might order this test when you have an infection and why the results influence treatment decisions.
Remember!
Key Points to Remember:
-
Bacteria trigger both innate responses (complement proteins, phagocytosis, neutrophil activation) and adaptive responses (antibodies for extracellular bacteria, cell-mediated immunity for intracellular bacteria). The gut microbiome provides crucial protection through colonisation resistance and quorum sensing.
-
Fungi are combated primarily by innate immunity (physical barriers, phagocytes with pattern recognition receptors) and cell-mediated adaptive immunity. Some fungi can evade immune detection, leading to chronic infections in approximately of cases.
-
Viruses require special immune strategies because they replicate inside cells. Infected cells display viral proteins on MHC class I molecules, allowing cytotoxic T cells to recognise and destroy them. Natural killer cells detect and eliminate cells with reduced MHC class I expression.
-
Protozoa and helminths use sophisticated evasion mechanisms including antigenic variation, intracellular hiding, and immunosuppression. Protozoal and helminth infections characteristically cause eosinophilia, while chronic infections indicate the parasite has successfully evaded immune clearance.
-
Full blood counts reveal characteristic patterns for different infections: neutrophilia suggests bacterial infection, leukopaenia often indicates viral infection, and eosinophilia points to parasitic infection. Understanding these patterns helps doctors diagnose and monitor infectious diseases effectively.