Disease Incidence and Prevalence (HSC SSCE Biology): Revision Notes
Disease Incidence and Prevalence
Introduction to disease surveillance
Tracking infectious diseases has become increasingly important in the modern world. Health authorities need accurate, real-time information to respond effectively to disease outbreaks and protect public health.
In Australia, both Federal and State/Territory governments work together to collect and analyse data on infectious diseases. Over the past century, this systematic approach has led to remarkable progress. Deaths from infectious diseases have dropped dramatically, from representing of all deaths a century ago to just in 2009.
However, the constant threat of new and emerging diseases, along with the re-emergence of diseases once thought controlled (such as tuberculosis, pertussis, and measles), means we need robust systems for gathering and analysing disease data.
Digital epidemiology: a new frontier
Digital epidemiology represents an exciting development in disease tracking. When people become ill, they often search the internet for information about their symptoms or share details on social media. Each online interaction is time-stamped and may include location data (geo-tagging). This creates the potential to track disease spread through populations in real time.
Whilst this promises to be valuable for disease surveillance, privacy concerns currently prevent its widespread implementation. For now, traditional data collection methods remain the primary approach.
Essential data for disease control
To effectively manage infectious diseases, health authorities must collect three key types of data:
Incidence and prevalence: These measurements determine the pool of pathogens already present in a population and help identify disease patterns.
Population mobility: This indicates how easily a pathogen can spread as people move between locations.
Immunisation rates: This shows what proportion of the population is vulnerable to infection and might act as carriers for the pathogen.
Incidence
Incidence measures the number of new cases of an infectious disease occurring during a specific time period. You can think of it as the infection rate, or the probability (risk) of contracting the disease.
Incidence is typically expressed as a percentage (number per 100) or as a number per 100,000 (or per 1,000 or 10,000) of the population.
Calculating incidence
To calculate disease incidence as a percentage, use this formula:
Worked Example: Calculating Incidence
A school has 1,000 students. During one week, 25 new cases of influenza appeared.
This means the risk of a student contracting influenza that week was , or there were new cases per 100 students in the population.
Exam tip: Incidence always refers to NEW cases only, not existing cases. Think of it as the "incoming" rate of disease.
Prevalence
Prevalence measures the proportion of a population that has a disease at a particular point in time. Unlike incidence, which counts only new cases, prevalence includes all cases - both newly diagnosed and previously existing ones. Prevalence is also expressed as a percentage.
Calculating prevalence
To calculate disease prevalence, use this formula:
Worked Example: Calculating Prevalence
A survey was conducted at the same school to count all students who had experienced influenza over the three winter months. The school had 1,000 students, and 150 students had contracted influenza during winter.
This means of the student population (or 15 out of every 100 students) had experienced influenza during winter.
Key distinction: Incidence measures the risk of getting the disease (new cases), whilst prevalence measures how widespread the disease is in the population (all cases).
Factors affecting disease spread
Population mobility
Population mobility is crucial when assessing potential disease outbreaks. Humans act as carriers for pathogens and can spread diseases to new locations when they travel.
The Australian Bureau of Statistics maintains detailed records on population movement, including:
- Interstate migration within Australia
- International migration rates
- Numbers of Australians travelling overseas by plane and boat each year
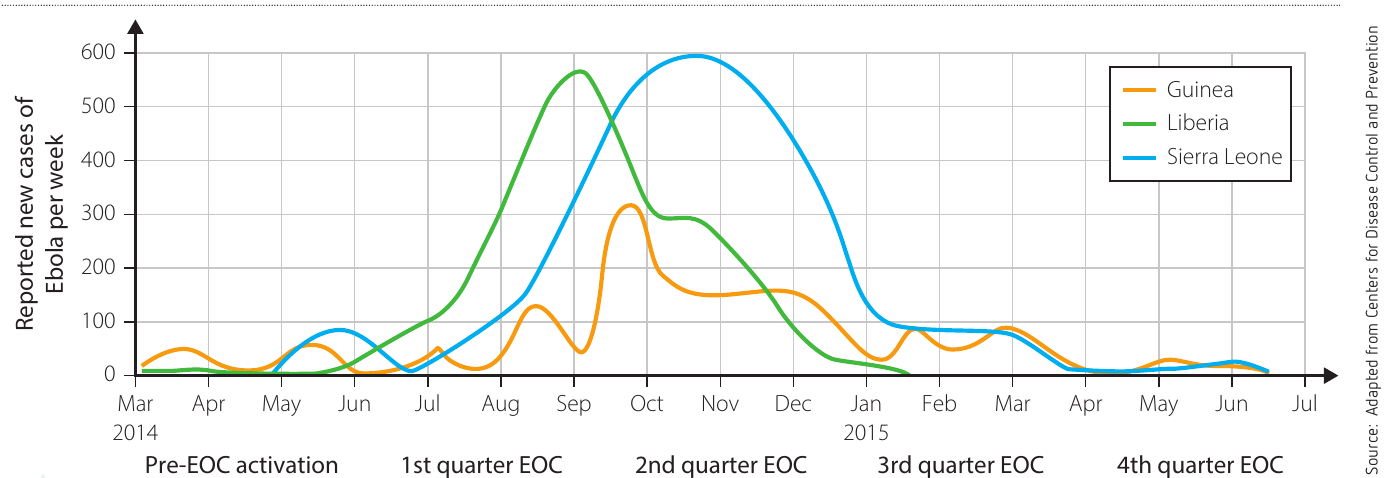
These mobility patterns are carefully monitored because they directly affect how quickly and widely a disease can spread. For example, in the Ebola outbreak shown in the graph above, population mobility played a critical role in both the spread and containment of the disease.
Immunisation and herd immunity
The immunisation rate of a population is a key factor in infectious disease control. The Australian Government's Immunise Australia Program works to promote and inform people about the value of immunisation in reducing disease transmission through communities.
When a significant proportion of a population has been immunised, this creates herd immunity. Herd immunity works by reducing the chances of unvaccinated individuals coming into contact with disease-causing microbes. When high numbers of people are vaccinated, the pathogen cannot spread easily through the population.
Importantly, herd immunity protects everyone in the population, including those who cannot be vaccinated (such as newborns, people with immune system disorders, or those allergic to vaccine components). This collective protection helps prevent epidemics.
Case study: malaria in Cambodia
Malaria remains one of the leading causes of death for children in South-East Asia. The disease is caused by the microbe Plasmodium falciparum, carried by various species of Anopheles mosquito vectors.
The following data shows malaria cases treated in Cambodia between 2000 and 2011:
| Year | Population (millions) |
|---|---|
| 2000 | 12.447 |
| 2005 | 13.358 |
| 2010 | 14.138 |
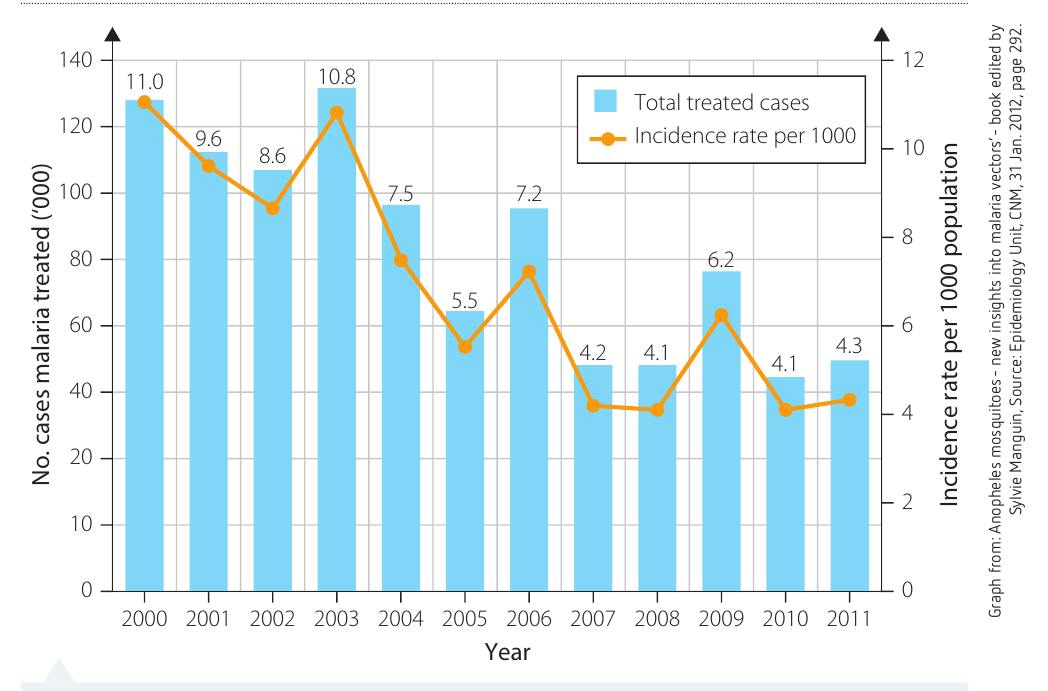
Analysing the trends
The graph shows that both the total number of malaria cases and the incidence rate per 1,000 population generally decreased over the period from 2000 to 2011. The data peaked in 2003 with an incidence rate of per 1,000 population, then dropped significantly by 2007-2008 to around per 1,000 population.
Several factors could explain this significant decrease:
- Implementation of effective mosquito control programmes
- Increased distribution of insecticide-treated bed nets
- Improved access to antimalarial medications
- Better public health education about prevention methods
- Enhanced disease surveillance and rapid treatment systems
Learning point: This case study demonstrates how tracking both incidence (new cases) and prevalence (total cases) over time helps public health authorities evaluate the effectiveness of disease control measures.
Key Points to Remember:
- Incidence measures the number of NEW cases occurring during a specific time period - it tells us the risk or rate of infection
- Prevalence measures ALL cases (both new and existing) in a population at a particular point in time - it tells us how widespread a disease is
- Both incidence and prevalence are typically expressed as percentages or as rates per 1,000 or 100,000 population
- Population mobility affects disease spread because people act as carriers when they travel to new locations
- Herd immunity occurs when high immunisation rates protect the entire population, including unvaccinated individuals, by reducing pathogen transmission
- Effective disease control requires monitoring incidence, prevalence, population mobility, and immunisation rates together