Technologies and Disorders (HSC SSCE Biology): Revision Notes
The Kidney
Introduction to the kidney
Kidneys are vital organs within the body's excretory system. They perform two essential functions: removing nitrogenous wastes from the bloodstream and maintaining optimal levels of substances such as salt and water through a process called osmoregulation.
The excretory system works continuously to keep your blood clean and your body's internal environment balanced. Without properly functioning kidneys, toxic waste products would accumulate in the blood, leading to serious health consequences.
The kidneys are so crucial to survival that the body is equipped with two of them. Even if one kidney fails, the other can perform enough filtration to sustain life, though with reduced capacity.
Structure and function of the kidney
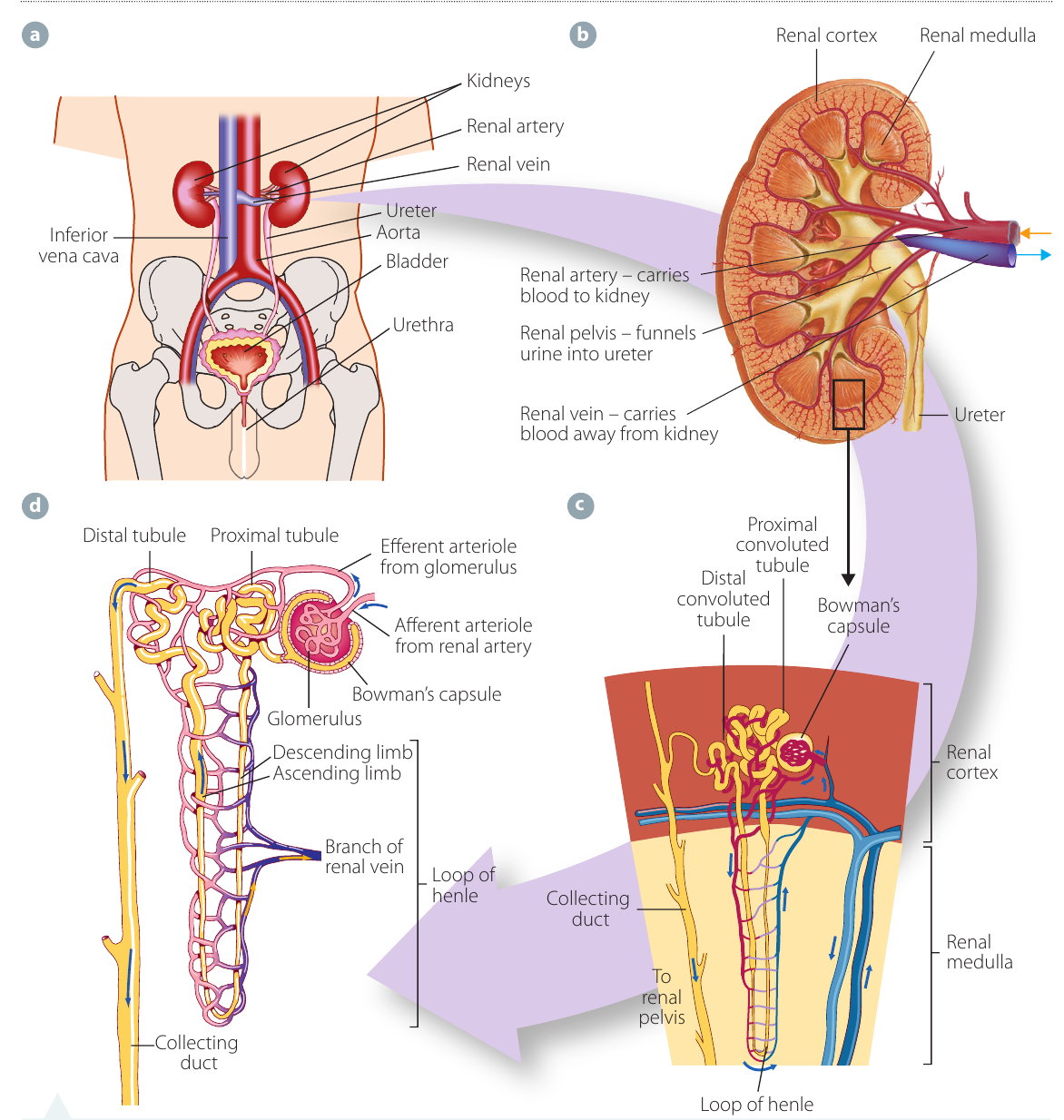
Three critical processes occur in the kidney: filtration, reabsorption, and secretion. To carry out these functions effectively, the kidney is organised into three main regions:
- Cortex: the outer layer of the kidney
- Medulla: the middle layer of the kidney
- Pelvis: the innermost funnel-shaped structure that collects urine
The nephron
The nephron is the functional unit of the kidney. Each kidney contains millions of these microscopic filtering units, which extend from the cortex down into the medulla. Understanding the nephron is crucial because this is where the actual work of blood filtering occurs.
Each nephron consists of several connected structures:
Bowman's capsule: A cup-shaped, double-walled hollow structure that serves as the starting point of the nephron. Inside this capsule sits the glomerulus.
Glomerulus: A ball-shaped network of tiny capillaries located within Bowman's capsule. Blood enters through the afferent arteriole and exits through the efferent arteriole.
Proximal tubule: The first section of the tubule immediately after Bowman's capsule, where most reabsorption occurs.
Loop of Henle: A U-shaped tubule that descends into the medulla and then ascends back up. It consists of a descending limb and an ascending limb.
Distal tubule: The final tubule section where fine-tuning of reabsorption and secretion occurs.
Collecting duct: The tube that receives fluid from multiple nephrons and carries it toward the renal pelvis.
Memory Aid: Remember the path through the nephron with "Big Boys Prefer Long Distances Collecting" - Bowman's capsule, Blood (glomerulus), Proximal tubule, Loop of Henle, Distal tubule, Collecting duct.
The following table shows which parts of the nephron are located in each kidney region:
| Region of kidney | Parts of nephron |
|---|---|
| Cortex | Glomerulus, Bowman's capsule, proximal tubule, distal tubule |
| Medulla | Loop of Henle, collecting duct |
The three main processes
Filtration
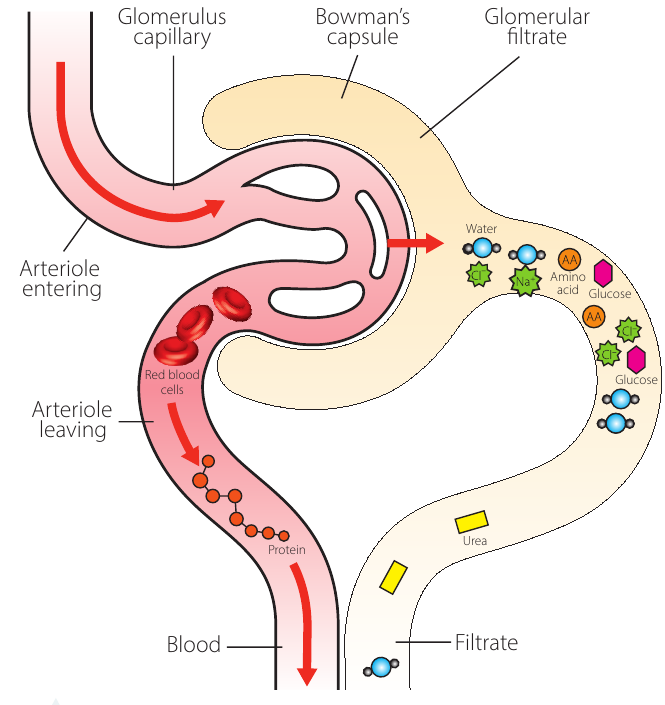
Filtration is the first step in urine formation and occurs at the junction between the glomerulus and Bowman's capsule.
Blood flows under high pressure from the heart through the aorta to the renal artery, which branches into increasingly smaller vessels. Eventually, millions of tiny capillaries form, each entering a nephron to become the glomerulus.
The high pressure forces blood against the walls of the glomerular capillaries. Because filtration is based on molecular size, all small molecules pass through the capillary walls into Bowman's capsule. This includes:
- Water ()
- Nitrogenous wastes (urea)
- Glucose
- Amino acids
- Various ions (salts such as , , )
Larger molecules cannot pass through and remain in the blood:
- Proteins
- Blood cells (red blood cells, white blood cells)
Critical Concept: Filtration is non-selective based on size alone. This means useful substances like glucose and amino acids are filtered out along with waste products. The kidney must later reclaim these valuable molecules through reabsorption.
Once inside Bowman's capsule, the filtered fluid is called glomerular filtrate. This filtrate continues its journey along the tubules that extend from the back of the capsule.
Reabsorption
Not everything that gets filtered out should leave the body. Reabsorption is the process of returning essential components from the filtrate back into the bloodstream.
The body reabsorbs many vital substances:
- All glucose
- All amino acids
- Most water ()
- Various ions: sodium (), potassium (), chloride (), calcium (), hydrogen bicarbonate ()
- Some vitamins
The rate at which different ions are reabsorbed varies depending on the body's needs, controlled through feedback mechanisms.
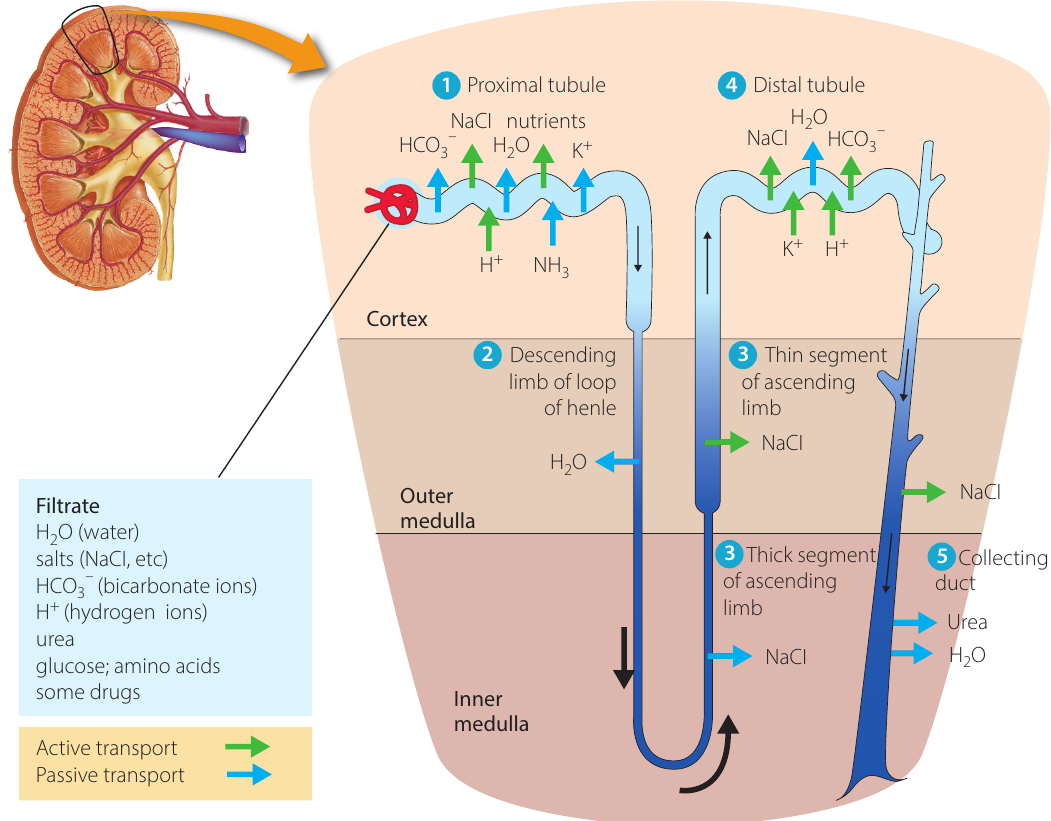
How reabsorption works:
Reabsorption occurs through two main processes:
- Active transport: Solutes (glucose, amino acids, ions) are actively pumped from the tubule back into surrounding blood capillaries. This occurs primarily in the proximal tubule and distal tubule.
- Passive transport (osmosis): As solutes are reabsorbed, the concentration of water in the tubule becomes higher than in the surrounding tissues. Water then follows by osmosis, moving from high to low water concentration.
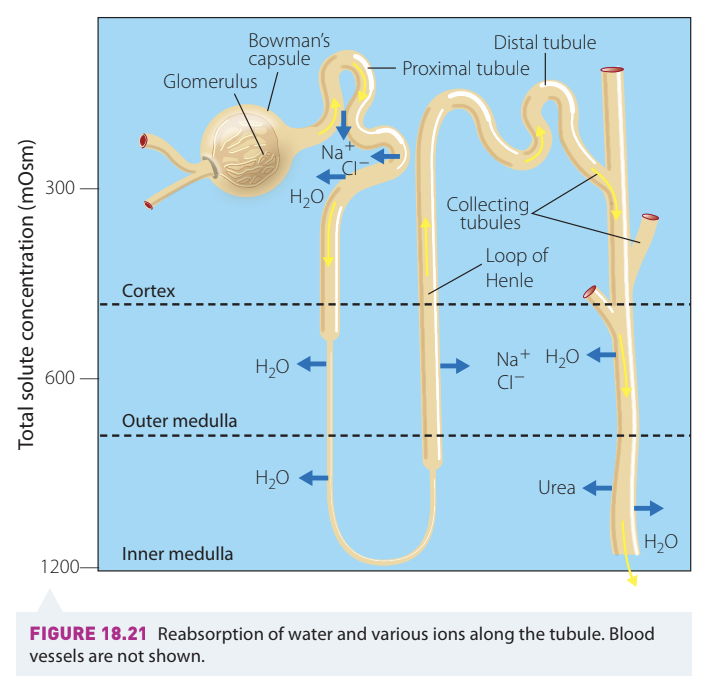
Special features of the Loop of Henle:
In the ascending limb of the Loop of Henle and the collecting duct, large numbers of sodium ions are actively pumped into the medulla tissues. This creates a concentration gradient that draws water out of the descending limb and collecting duct by osmosis.
Key Feature: The ascending limb of the Loop of Henle is impermeable to water, so only ions move here, not water. This creates the concentration gradient needed for water reabsorption elsewhere in the nephron.
Importantly, the ascending limb of the Loop of Henle is impermeable to water, so only ions move here, not water. This creates the concentration gradient needed for water reabsorption elsewhere.
Most urea and other waste products are not reabsorbed, remaining in the tubule to be eliminated.
Secretion
Secretion (also called tubular secretion) is the third process contributing to urine formation. While filtration moves substances from blood to tubule based on size, secretion actively moves specific toxic substances from the blood and surrounding tissues into the tubules for removal.
Substances secreted include:
- Metabolic wastes: urea, uric acid, ammonia (), hydrogen ions ()
- Drugs: penicillin, morphine, saccharin
Where secretion occurs:
- Proximal tubule: Hydrogen ions (), drugs (penicillin, morphine, saccharin)
- Descending limb of Loop of Henle: Urea (note: the ascending limb and distal tubules are impermeable to urea)
The movement of urea and ammonia occurs mainly through diffusion, whilst other substances require active transport.
Understanding Secretion: Think of secretion as the kidney's "second chance" to remove harmful substances. While filtration catches most waste products based on size, secretion specifically targets and removes toxins that may have escaped filtration or are produced by surrounding tissues.
Hormonal regulation of osmoregulation
Two important hormones regulate kidney function:
Aldosterone: This hormone stimulates the reabsorption of salt (primarily sodium chloride) in the Loop of Henle. By controlling salt reabsorption, aldosterone helps regulate both salt and water balance in the body.
Antidiuretic hormone (ADH), also called vasopressin: This hormone stimulates water reabsorption in the kidney. When ADH levels are high, more water is reabsorbed and urine becomes more concentrated. When ADH levels are low, less water is reabsorbed and urine becomes more dilute.
Memory Aid: Remember "AAAldosterone for sAAAlt" and "ADH for wAAAter" - Aldosterone controls salt reabsorption, while ADH (Antidiuretic Hormone) controls water reabsorption.
Urine formation and removal
After filtration, reabsorption, and secretion are complete, the remaining fluid in the collecting duct is called urine. Urine consists of:
- Water
- Nitrogenous wastes (primarily urea)
- Other waste products
- Excess ions
Urine collects in the renal pelvis at the centre of the kidney. From there, it flows through the ureters (one from each kidney) to the bladder for storage. When the bladder is full, urine is eliminated from the body through the urethra.
Loss of kidney function
Symptoms of kidney disease
Loss of kidney function often develops gradually, with few noticeable signs until significant damage has occurred. When nephrons are damaged, they cannot properly filter, reabsorb, and secrete substances. This leads to a dangerous build-up of wastes and an inability to balance water and salt levels in the blood.
Warning Signs: Kidney disease is often called a "silent" disease because symptoms may not appear until 75-80% of kidney function is lost. Regular health check-ups are essential for early detection.
Common symptoms include:
- Nausea and vomiting
- Loss of appetite
- Fatigue and weakness
- Sleep disturbances
- Changes in urine volume (producing more or less than normal)
- Decreased mental sharpness
- Muscle twitches and cramps
- Swelling of feet and ankles (oedema)
- Persistent itching
- Chest pain (if fluid accumulates around the heart lining)
- Shortness of breath (if fluid builds up in the lungs)
- High blood pressure (hypertension) that is difficult to control
Causes of kidney disease
Several conditions can damage nephrons and reduce kidney function:
Diabetes (Type 1 and Type 2): High blood glucose levels force the kidneys to filter more blood than normal, placing stress on the nephrons. Over time, nephrons become damaged and large molecules such as proteins begin to "leak" through into the tubules. These proteins cause blockages, leading to further nephron damage.
Chronic high blood pressure (hypertension): The constant high pressure of blood being forced through the glomerular capillaries causes physical damage to the nephron walls. Large molecules leak into the tubules, causing blockages and reducing the nephrons' ability to function effectively.
Recurrent kidney infections: Repeated infections damage nephrons directly. Additionally, prolonged use of certain medications to treat these infections can further reduce kidney function.
Blockages: Kidney stones, tumours, or anything blocking the passage of urine causes urine to "back up" into the kidney. The resulting pressure buildup will cause kidney damage and, if the blockage is not removed, complete kidney shutdown.
How Diabetes Damages Kidneys:
Step 1: High blood glucose levels require increased filtration
- The kidneys work harder to filter excess glucose from the blood
Step 2: Increased pressure damages glomerular walls
- Continuous high-pressure filtration weakens the capillary walls
Step 3: Proteins leak through damaged walls
- Large protein molecules that should stay in the blood pass into the tubules
Step 4: Protein blockages damage nephrons
- Accumulated proteins clog tubules, causing progressive nephron failure
Technology to assist with kidney failure
When kidneys fail, toxic metabolic wastes accumulate in the blood because there is no natural way to remove them. Without treatment, this toxicity eventually leads to death.
Renal dialysis has been developed to artificially perform some kidney functions, allowing blood to be filtered even when the kidneys are severely damaged. There are two types of renal dialysis: haemodialysis and peritoneal dialysis.

Haemodialysis
In haemodialysis, the patient is connected to a dialysis machine that filters their blood externally.
How haemodialysis works:
The patient's blood is pumped through a system of tubes that have artificial semi-permeable membranes. These tubes are coiled to increase their surface area, which speeds up the rate of diffusion. The tubes are submerged in dialysate (dialysis fluid).
The dialysate flows in the opposite direction to the blood flow. This counter-current flow maintains a concentration gradient to maximise the rate of diffusion.
The Dialysate Solution: The dialysate has the same composition as blood plasma but without the metabolic wastes. Because waste concentration is higher in the blood than in the dialysate, metabolic wastes move through the semi-permeable membrane into the dialysing fluid by diffusion.
The dialysate has the same composition as blood plasma but without the metabolic wastes. Because waste concentration is higher in the blood than in the dialysate, metabolic wastes move through the semi-permeable membrane into the dialysing fluid by diffusion. The dialysate must be continuously replaced to maintain the concentration gradient.
Limitations of haemodialysis:
- Time-consuming: requires 3-4 hours of treatment, 2-3 times per week
- Limited efficiency: only limited amounts of fluid and wastes can be removed from the blood
- Poor ion regulation: substances such as sodium phosphate and potassium ions do not diffuse quickly enough and may accumulate in the blood
- Dietary restrictions: patients must follow a specific diet to prevent dangerous ion accumulation
Critical Limitation: While haemodialysis can successfully filter waste products from blood, it cannot replace all kidney functions. It does not produce hormones like a healthy kidney does, and the regulation of water and salt balance is less precise than natural kidney function.
Peritoneal dialysis
Peritoneal dialysis uses the patient's own abdominal cavity as the filtering system.
How peritoneal dialysis works:
Dialysate is introduced into the patient's abdominal cavity through a catheter. The peritoneal membrane (the lining of the abdominal cavity) acts as a natural semi-permeable membrane. Waste products diffuse from blood vessels in the peritoneal membrane into the dialysate. After several hours, the fluid containing the wastes is drained out and replaced with fresh dialysate.
This method can be done at home and offers more flexibility than haemodialysis, but it carries a risk of infection and may not be suitable for all patients.
Comparing Dialysis Methods:
- Haemodialysis: Performed at a medical facility, requires 3-4 hours per session, 2-3 times weekly
- Peritoneal dialysis: Can be done at home, requires multiple exchanges throughout the day or overnight, offers more flexibility but higher infection risk
Investigation: identifying kidney regions
A practical investigation involves examining the external and internal structure of a mammalian kidney through dissection or virtual models. This helps consolidate understanding of kidney anatomy.
External structures to identify:
- Adipose tissue (fat) surrounding the kidney
- Renal capsule (protective covering)
- Hilum (curved indentation where vessels enter/exit)
- Renal artery (brings blood to kidney)
- Renal vein (carries filtered blood away)
- Ureter (carries urine to bladder)
Internal structures to identify:
- Cortex (outer, darker region containing glomeruli and Bowman's capsules)
- Medulla (middle, lighter region organised into pyramids containing loops of Henle and collecting ducts)
- Renal pyramids (triangular sections in the medulla)
- Calyces (cup-like structures that collect urine from pyramids)
- Renal pelvis (central cavity where urine collects before entering the ureter)
Language Note: The adjective used to describe anything associated with the kidney is renal - for example, renal artery, renal vein, renal failure.
Key Points to Remember:
-
The kidney's main functions are excreting nitrogenous wastes and maintaining water and salt balance (osmoregulation).
-
The three kidney regions are the cortex (outer), medulla (middle), and pelvis (inner collecting area).
-
The nephron is the functional unit of the kidney, consisting of the glomerulus, Bowman's capsule, proximal tubule, Loop of Henle, distal tubule, and collecting duct.
-
Three key processes occur: filtration (size-based filtering at the glomerulus), reabsorption (returning essential substances to the blood), and secretion (actively removing additional toxins).
-
Two hormones regulate kidney function: Aldosterone controls salt reabsorption, while ADH controls water reabsorption.
-
Kidney disease is often caused by diabetes, hypertension, or infections, which damage nephrons and reduce kidney function.
-
When kidneys fail, dialysis can artificially filter the blood, though it is time-consuming and has limitations compared to healthy kidneys.