Control of Infectious Diseases (OCR A-Level Biology A): Revision Notes
Control of Infectious Diseases
Vaccination programmes
Governments provide vaccination programmes as a key health protection measure for their populations. Young children receive vaccines against diseases that were once widespread and caused significant illness and death.
The UK follows a structured vaccination schedule:
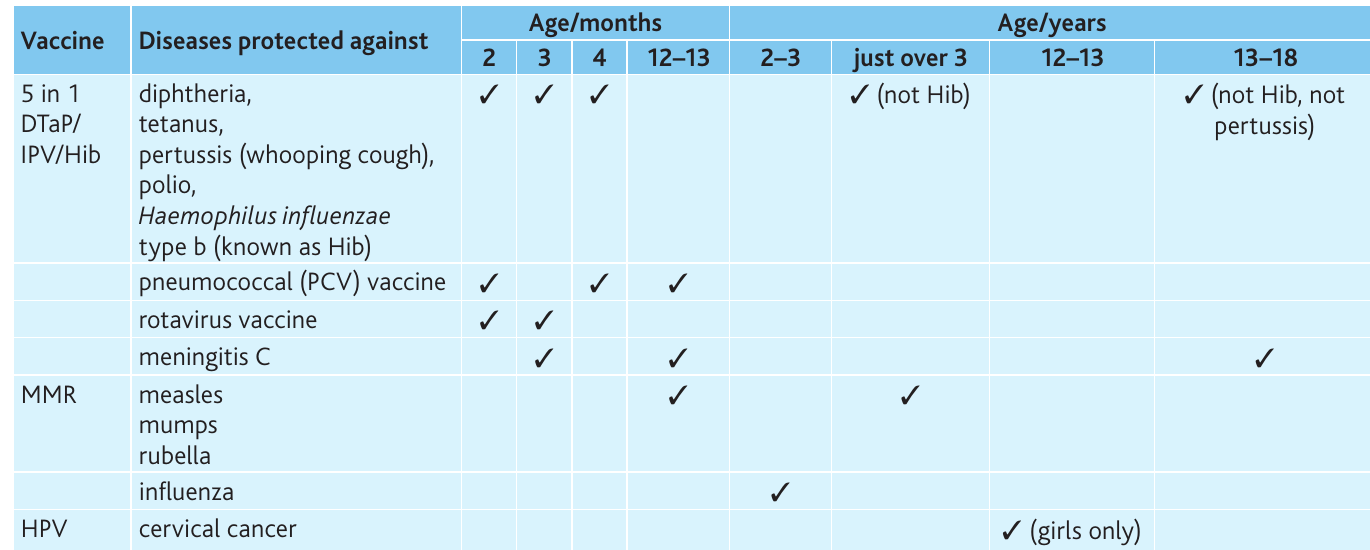
Although many of these diseases are now rare in the UK, they remain threats. Polio, for example, has not occurred naturally in the UK since , but the disease persists globally. In , Pakistan recorded 93 cases, and as of , polio remained endemic in Pakistan, Afghanistan, and Nigeria. The World Health Organization (WHO) continues working toward complete eradication of this disease.

The term immunisation encompasses both artificial active immunity (vaccination) and artificial passive immunity. It is not synonymous with vaccination alone.
Strategies for disease eradication
Vaccination programmes employ two main approaches during eradication campaigns:
Herd immunity
Herd immunity develops when vaccination coverage reaches very high levels across a population. When the majority of people are vaccinated, pathogen transmission becomes extremely difficult because most individuals cannot harbour or spread the disease. This protects vulnerable people who cannot be vaccinated or do not respond to vaccines, as their exposure risk is minimal.
Programmes typically aim for close to 100% coverage to establish effective herd immunity. This high threshold ensures that even those who cannot be vaccinated (such as immunocompromised individuals or infants) are protected by the immunity of the surrounding population.
Ring immunity
Ring immunity involves vaccinating people in close proximity to an infected individual—those living or working nearby, or their contacts. This creates a protective barrier that prevents disease spread beyond the initial case.
Challenges in vaccine development
Eukaryotic pathogens
Developing vaccines against diseases caused by eukaryotic organisms presents significant challenges. The malarial parasite Plasmodium exemplifies these difficulties:
Why Malaria Vaccine Development Is So Challenging:
- It possesses numerous genes encoding different cell surface antigens
- Different strains express different antigens
- During its life cycle stages in liver and red blood cells, it expresses changing antigens
- The parasite remains inside host cells, where antibodies cannot reach it
These characteristics make it extremely difficult to develop a vaccine that provides comprehensive protection against malaria.
Viral variation
The influenza virus poses particular challenges due to its ability to change surface antigens through three mechanisms:
Antigenic drift: Small modifications in antigen structure and shape within the same viral strain.
Antigenic shift: Major changes in antigens within the same strain.
Cross-breeding: Different viral strains simultaneously infect a cell, producing new viruses with mixed antigens from both parent strains.
Human influenza viruses may cross-breed with animal viruses, or animal strains may cross the species barrier. The twentieth century saw three major influenza pandemics, with Spanish flu following World War I being the most devastating. The most recent pandemic was swine flu in .

The WHO and national governments monitor for new viral strains that could cause pandemics. Each year, the WHO provides guidance on likely circulating strains, enabling vaccine preparation and distribution. High-risk individuals in the UK receive annual influenza vaccination.
Health authorities maintain stockpiles of antiviral drugs such as oseltamivir (Tamiflu) and zanamivir (Relenza). These drugs inhibit viral release from infected cells. However, questions remain about whether sufficient vaccine or drug supplies could be produced quickly enough to prevent a pandemic comparable to .
The WHO estimates that 30 new diseases have emerged over the past years, including HIV/AIDS, SARS, ebola, West Nile disease, and Lyme disease. Few effective antiviral drugs exist.
Antibiotics
An antibiotic is any substance produced by a microorganism that, in dilute solution, harms or kills another microorganism.
Most antibiotics originate from actinobacteria, particularly Streptomyces species. Examples include streptomycin, erythromycin, and tetracycline. Some antibiotics, like penicillin, come from fungi such as Penicillium. Many modern antibiotics are semi-synthetic—produced by microorganisms in fermenters, then chemically modified, or entirely synthesised chemically.
Mechanism of action
How Penicillin Works:
Penicillin, one of the first mass-produced antibiotics, works by inhibiting the bacterial enzyme transpeptidase. This enzyme catalyses murein synthesis for bacterial cell walls. Without protective cell walls, bacteria absorb water, swell, and burst.
Antibiotics only function if they can:
- Enter bacterial cells
- Find a suitable target to inhibit
Broad-spectrum antibiotics affect many bacterial types, whilst narrow-spectrum antibiotics target only specific bacteria.
Antibiotic resistance
Shortly after antibiotics became widely available, doctors observed that some previously treatable infections no longer responded. Bacteria had developed resistance.
Development of resistance
How Resistance Develops:
When a person takes antibiotics, susceptible bacteria die. If treatment is incomplete—for example, if patients stop taking antibiotics when symptoms disappear—some bacteria may survive. Mutations can then confer resistance, making future infections harder to treat.
This is why it is critical to complete the full course of antibiotics, even if you feel better before finishing the medication.
Bacteria carry single copies of genes in their circular DNA, meaning mutant genes have immediate effects. Bacteria with resistance genes gain a selective advantage: whilst susceptible bacteria die, resistant ones survive and reproduce rapidly. A single resistant bacterium can produce 10,000 million descendants within 24 hours.
Mechanisms of resistance
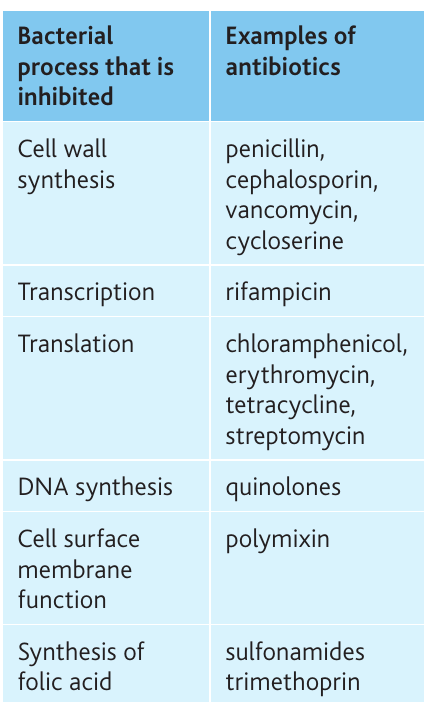
Resistance genes, often located on plasmids, spread easily between bacteria—even across species. These genes may code for:
- Penicillinase: an enzyme that breaks down penicillin
- Modified enzymes for DNA synthesis, rendering quinolones ineffective
- Membrane 'pumps' that actively remove antibiotics like tetracyclines from cells
- Modified ribosome structures preventing antibiotic binding (e.g., resistance to erythromycin)
- Altered cell wall structures making antibiotics like cycloserine ineffective
- Modified membrane components reducing antibiotic entry
Hospital-acquired infections
Multi-drug-resistant strains are particularly prevalent in hospitals, where antibiotic use is heavy and patients often have weakened immune systems.
MRSA (methicillin-resistant Staphylococcus aureus) represents a significant concern. S. aureus normally colonises human skin and airways without problems, but can cause disease if it enters the body through wounds or medical procedures. Resulting infections range from mild skin infections to life-threatening conditions including:
- Infected wounds and eczema
- Abscesses and joint infections
- Heart valve infections
- Pneumonia
- Bacteraemia (bloodstream infection)
Whilst most S. aureus strains respond to common antibiotics, MRSA requires different treatment approaches. MRSA and MSSA (methicillin-susceptible S. aureus) differ only in antibiotic resistance.
Clostridium difficile (C. diff) normally inhabits the gut under control of other bacteria. When antibiotic treatment kills these beneficial bacteria, C. difficile populations may increase, releasing toxins that disrupt intestinal epithelium function, causing diarrhoea and fever. Symptoms can be severe in elderly patients.
Cases of MRSA and C. difficile increased significantly in the late s and s. Between and , hospital MRSA infections halved in the USA and decreased by 80% in England. Similar reductions occurred with C. difficile. These improvements resulted from enhanced hygiene practices: frequent hand washing and thorough surface cleaning with bleach.
Drug-resistant tuberculosis
Since antibiotic treatment began in the s, drug-resistant strains of Mycobacterium tuberculosis have emerged. Antibiotics act as selective agents, eliminating susceptible bacteria whilst resistant strains survive.
Resistance develops through random DNA mutations, occurring at approximately one in every thousand bacteria. Using three drugs simultaneously reduces resistance probability to one in a thousand million; four drugs reduce it to one in a billion. This reasoning underlies combination therapy for tuberculosis.
Direct Observation Treatment, Short Course (DOTS):
The WHO promotes DOTS, where health workers or family members ensure patients take medication regularly for six to eight months. This approach helps ensure treatment completion and reduces the development of drug-resistant strains.
The four front-line TB drugs (isoniazid, pyrazinamide, rifampicin, and ethambutol) used together cure 95% of patients and help reduce multi-drug-resistant (MDR) strain spread.
Why Completing TB Treatment Is Critical:
Incomplete treatment or premature cessation allows bacteria to spread throughout the body, increasing mutation likelihood. People who do not complete treatment may develop bacteria resistant to all drugs being used and can easily infect 10–15 others, especially in overcrowded conditions.
Two forms of drug-resistant TB exist:
- MDR-TB: resistant to at least isoniazid and rifampicin (the two main TB drugs)
- XDR-TB (extensively drug-resistant TB): resistant to first-line drugs and drugs used against MDR-TB; particularly threatens HIV-positive individuals
Resistant TB strains do not respond to standard six-month first-line treatment and may require two years or more of treatment with less effective, more expensive drugs.
In , approximately 450,000 people worldwide developed MDR-TB, with an estimated being XDR-TB cases.
Sources of new medicines
No new antibiotic class has been discovered since 1987. Scientists continue searching for new antibiotics amid concerns that previously curable diseases may return untreatable.
Discovery methods
New drugs are developed through several approaches:
- Identifying promising compounds from organisms (fungi, actinobacteria, plants, animals)
- Genetic analysis to find genes potentially coding for useful drugs
- Finding molecules that fit drug targets (e.g., hormone receptors, neurotransmitter receptors at synapses)
- Modifying existing drugs using computer modelling of molecular structures and targets
Examples of promising sources
Marine Actinobacteria:
Marine actinobacteria produce rifamycins—antibiotics effective against bacteria by inhibiting transcription. Some actinobacteria live on or inside marine animals, demonstrating how unexplored ecosystems can provide new medicinal compounds.
Rainforest Plants:
Calophyllum lanigerum, a rare Malaysian rainforest tree, produces calanolide A, which prevents HIV entering T helper cell nuclei. This stops T helper cells producing new viruses, decreasing HIV spread throughout the body.
Plant-derived medicines
Traditional medicines provide excellent potential sources, as many current drugs derive from plants:
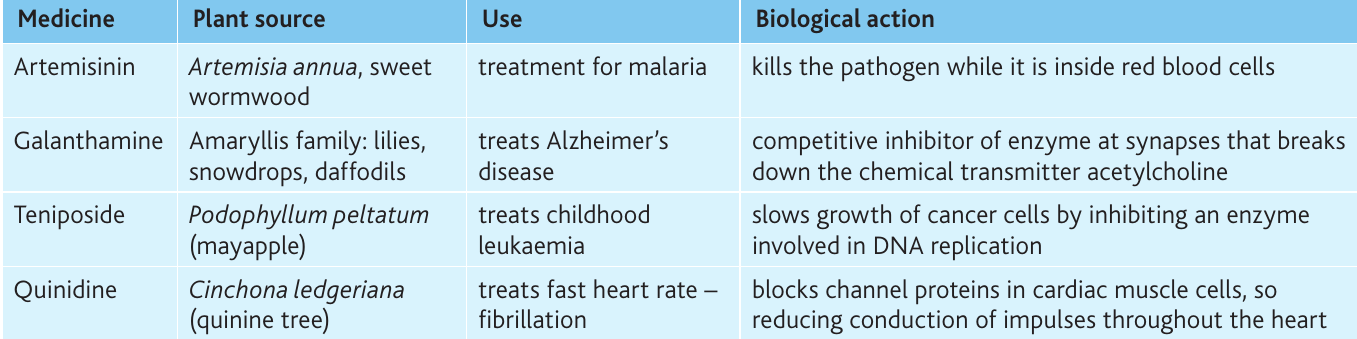

Cinchona ledgeriana also produces quinine, the first antimalarial drug, still used for severe Plasmodium falciparum cases.
Many drugs originate from organism studies. Antibiotics come from fungi and bacteria; anti-cancer drugs from plants like vinblastine from Madagascan periwinkle (Catharantus roseus) and taxol from Pacific yew (Taxus brevifolia). Current research catalogues Chinese medicinal plants for potential mass-produced drugs like artemisinin.
Conservation and Medicine:
Conserving species at extinction risk is important for many reasons, but potential drug provision presents a powerful utilitarian argument for maintaining biodiversity. Undiscovered species may hold the key to treating currently incurable diseases.
Drug development requires extensive time and funding, involving lengthy trialling periods and approval by national regulatory authorities.
Personalised medicines
Doctors have long recognised that identical medicines show varying effectiveness between patients. For example, people treated with isoniazid for TB divide into:
- Slow metabolisers: effective treatment
- Fast metabolisers: minimal benefit
These differences relate to genetic variation affecting protein structures. Drug targets vary between individuals due to genetic differences in protein-coding genes.
Personalised medicines involve testing individual genomes to identify which drugs will be effective for specific patients. Rather than prescribing identical drugs for everyone, doctors can prescribe medications known to be suitable based on genomic information. This ensures more precise treatment, avoiding adverse effects and improving efficacy.
Cancer Treatment with Trastuzumab:
Trastuzumab (Herceptin) is an antibody drug interfering with specific cell surface receptors, used primarily for certain breast cancers. It is only prescribed after testing confirms the cancer has high receptor numbers. This approach ensures treatment effectiveness while avoiding unnecessary side effects in patients who would not benefit.
Synthetic biology
In May , scientists announced assembling a complete genome of millions of base pairs, inserting it into an enucleated bacterial cell, and causing that cell to replicate DNA and divide. These first synthetic cells cost over $ million to create.
This goes beyond genetic engineering to produce one or two new products—it involves assembling genomes to operate cells in entirely new ways. Genomes can be assembled from existing DNA sequences plus new sequences written to produce specific proteins or control genes in specific ways.
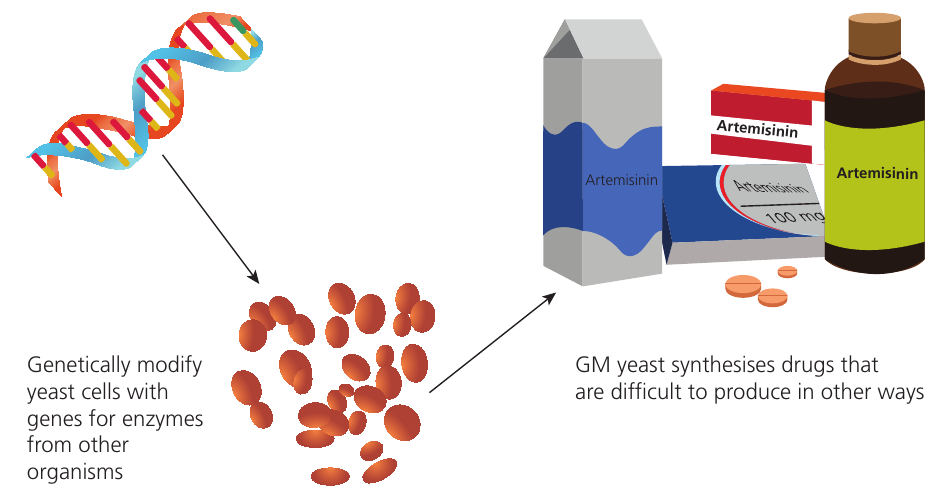
What Is Synthetic Biology?
Synthetic biology offers potential for developing new drugs requiring complex synthesis difficult or expensive to achieve chemically. A well-known application is genetically modifying E. coli and yeasts for commercial production of an artemisinin precursor.
The Urgent Need for New Antimalarials:
Recently, healthcare workers in Cambodia and Myanmar observed signs that Plasmodium is developing artemisinin resistance. This raises urgent questions about future antimalarial drug sources and highlights the critical importance of ongoing drug development.

Key Points to Remember:
- Vaccination programmes create herd immunity and ring immunity, protecting populations by reducing pathogen transmission opportunities.
- Vaccine development challenges include eukaryotic pathogens with multiple antigens and rapidly evolving viruses showing antigenic drift and shift.
- Antibiotic resistance develops through bacterial mutations and gene transfer, with incomplete treatment courses accelerating resistance spread.
- Multi-drug-resistant strains like MRSA and C. difficile require improved hygiene practices and careful antibiotic use to control.
- New medicine sources include marine organisms, rainforest plants, and synthetic biology approaches, highlighting the importance of biodiversity conservation.
- Personalised medicines use genetic testing to match effective drugs to individual patients, improving treatment outcomes and reducing side effects.