The Mechanism of Ventilation and Breathing Measurements (OCR A-Level Biology A): Revision Notes
The Mechanism of Ventilation and Breathing Measurements
Introduction to ventilation
Breathing, or ventilation, keeps the air in the alveoli fresh. This process is essential because gas exchange requires concentration gradients. Oxygen concentration must remain higher in the alveoli than in the blood, whilst carbon dioxide concentration must stay lower in the alveoli than in the blood. Without ventilation, these gradients would disappear and gas exchange would cease.
The maintenance of concentration gradients is absolutely critical for gas exchange. If these gradients collapse, oxygen cannot diffuse into the blood and carbon dioxide cannot diffuse out, regardless of how well-designed the alveolar structure is.
Ventilation occurs through the coordinated action of two main structures: the intercostal muscles (located between the ribs) and the diaphragm (a sheet of muscle forming the floor of the thoracic cavity). The natural elasticity of the lungs also plays an important role, though the lungs themselves respond passively to pressure changes around them.
How breathing works
The pressure-volume relationship
Understanding breathing requires knowledge of how pressure and volume relate in air-filled spaces. An inverse relationship exists between these two variables:
- When volume increases, pressure decreases
- When volume decreases, pressure increases
This pressure-volume inverse relationship is the fundamental principle underlying all breathing movements. Every aspect of ventilation—from the smallest breath to the deepest inhalation—relies on this physical law.
This principle explains why air moves in and out of the lungs. The diaphragm and intercostal muscles alter the volume of the thoracic cavity, which changes the pressure inside the lungs relative to atmospheric pressure outside the body.
Inspiration
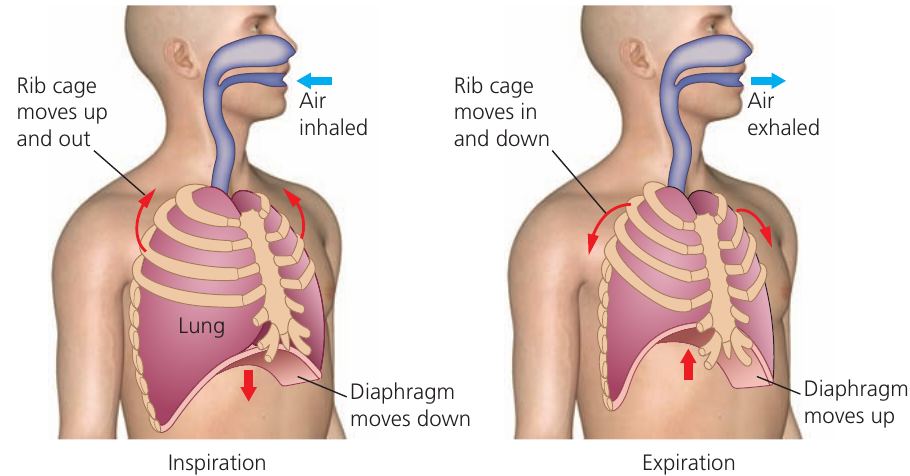
Inspiration (also called inhalation) is the active process of drawing air into the lungs. It occurs through the following sequence:
- The inspiratory center in the medulla oblongata (part of the brain) sends nerve impulses to the breathing muscles
- The external intercostal muscles contract, pulling the rib cage upwards and outwards
- Simultaneously, the diaphragm contracts and flattens, moving downward
- These movements increase the volume of the thoracic cavity
- The increased volume causes pressure inside the lungs to fall below atmospheric pressure
- Air flows in from outside (where pressure is higher) until pressures equalise
- The inflowing air causes the lungs to expand
During inspiration, stretch receptors in the lung tissue detect the expansion and send signals back to the brain.
Expiration
Expiration (also called exhalation) removes air from the lungs. In normal breathing at rest, expiration is a passive process:
- The inspiratory center stops sending nerve impulses
- The external intercostal muscles relax, allowing the rib cage to move downward and inward
- The diaphragm relaxes and moves upward, returning to its domed shape
- These movements decrease the volume of the thoracic cavity
- The natural elasticity of the lungs causes them to recoil
- The decreased volume causes pressure inside the lungs to rise above atmospheric pressure
- Air flows out (where pressure is lower) until pressures equalise
Passive vs Active Expiration
Normal expiration at rest requires no muscular effort—it happens automatically when the inspiratory muscles relax and the elastic lungs recoil. This energy-efficient design means we don't have to consciously work to breathe out during quiet breathing.
However, during forced expiration (such as when blowing out forcefully or during vigorous exercise), an additional set of muscles becomes active. The internal intercostal muscles contract, pulling the rib cage down and in more forcefully. This increases pressure on the lungs beyond what natural elasticity alone provides. An expiratory center in the brain controls these muscles.
Control of the breathing cycle
The complete breathing cycle involves precise coordination:
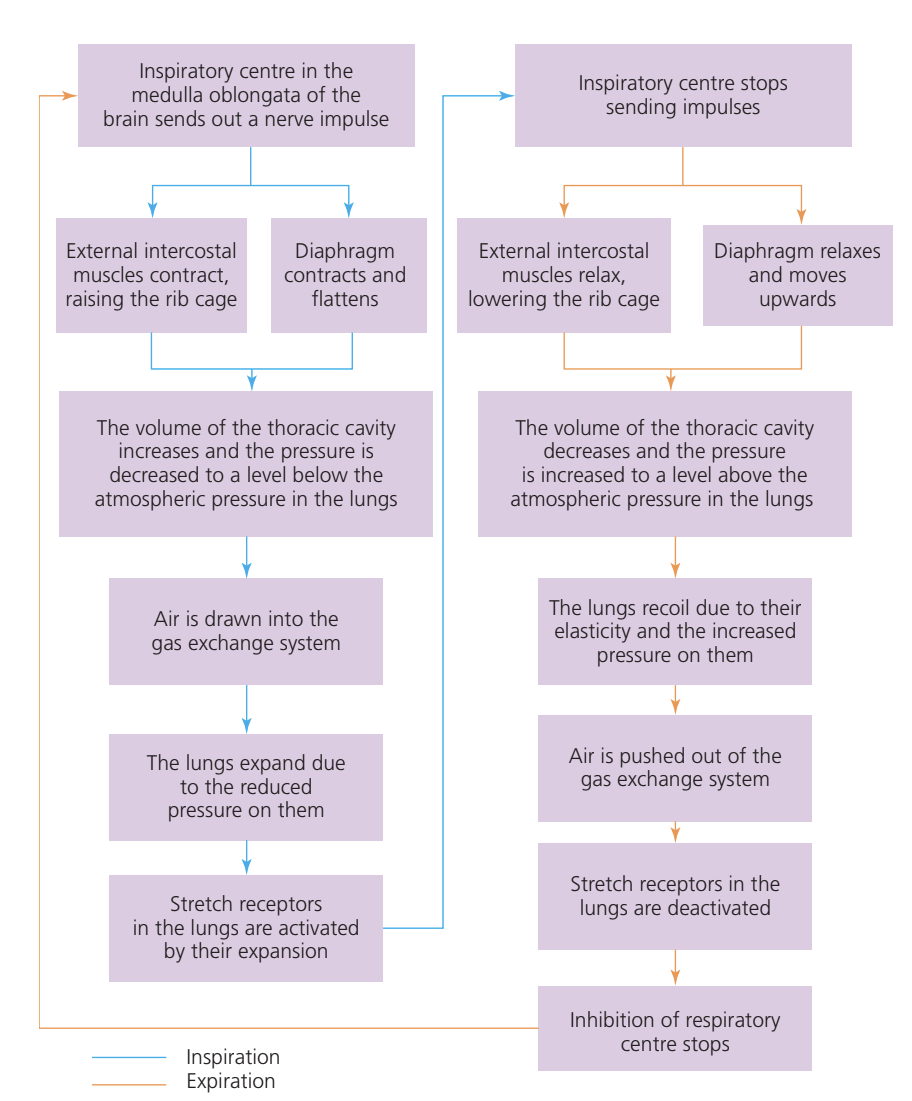
The flowchart above illustrates how inspiration and expiration alternate. Stretch receptors provide crucial negative feedback: when the lungs expand sufficiently during inspiration, these receptors signal the inspiratory center to stop sending impulses. This halts inspiration and allows expiration to begin. When the stretch receptors are no longer stimulated (because the lungs have deflated), the inhibition stops and the cycle restarts.
Measuring breathing with spirometry
Spirometry equipment
A spirometer is a device that measures various aspects of breathing. The subject breathes in and out through a mouthpiece connected to a sealed chamber, whilst wearing a nose clip to ensure all air passes through the apparatus.
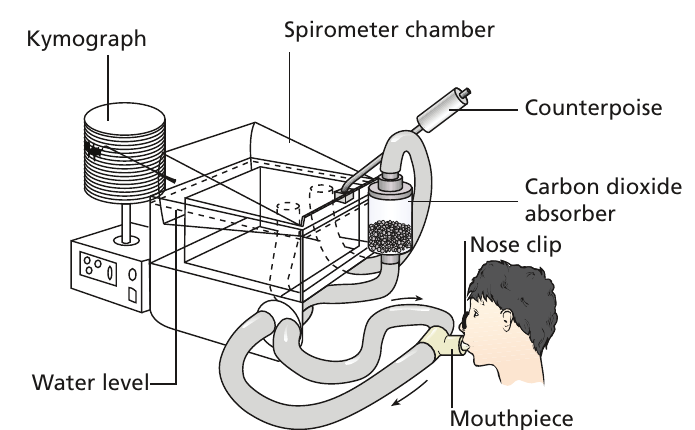

The spirometer chamber floats on water and moves up when the subject breathes out, and down when they breathes in. These movements are recorded either on a revolving drum (called a kymograph) or displayed electronically on a screen.
Safety Feature: Carbon Dioxide Removal
An essential safety component is the carbon dioxide absorber containing soda lime. As the subject re-breathes the air in the chamber, carbon dioxide must be removed to prevent respiratory distress. Without this, the accumulation of would cause discomfort and potentially harm the subject.
Key breathing measurements
A spirometer can measure several important volumes:
Key Spirometry Measurements
-
Vital capacity: The maximum volume of air that can be breathed in or out in a single breath. This represents the greatest change in lung volume that a person can achieve voluntarily.
-
Tidal volume: The volume of air normally breathed in or out during quiet breathing at rest. This is much smaller than vital capacity and represents typical, relaxed breathing.
-
Breathing rate: The number of breaths per minute. One breath consists of both breathing in and breathing out. The unit is written as breaths min.
-
Oxygen uptake: The amount of oxygen consumed by the subject. Because the spirometer removes but the subject continues extracting , the total volume of air gradually decreases. The rate of this decrease indicates how quickly oxygen is being used.
Residual volume is a small volume of air that always remains in the lungs, even after the most forceful exhalation. A spirometer cannot measure this volume because the subject cannot expel it.
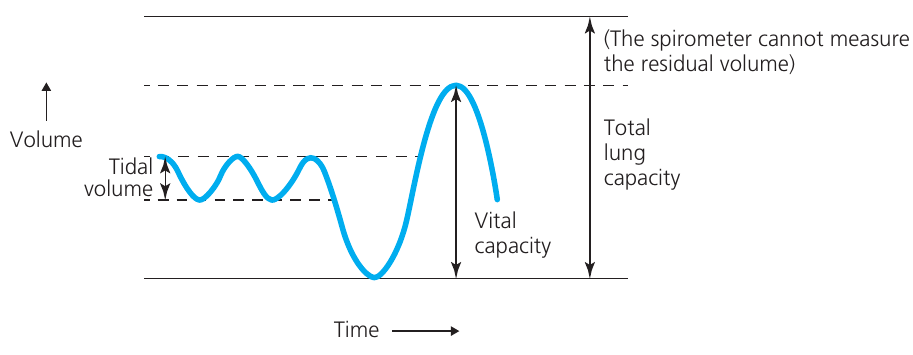
The diagram above shows how these different volumes appear on a spirometer trace. The total lung capacity equals the vital capacity plus the residual volume.
Analyzing spirometer traces
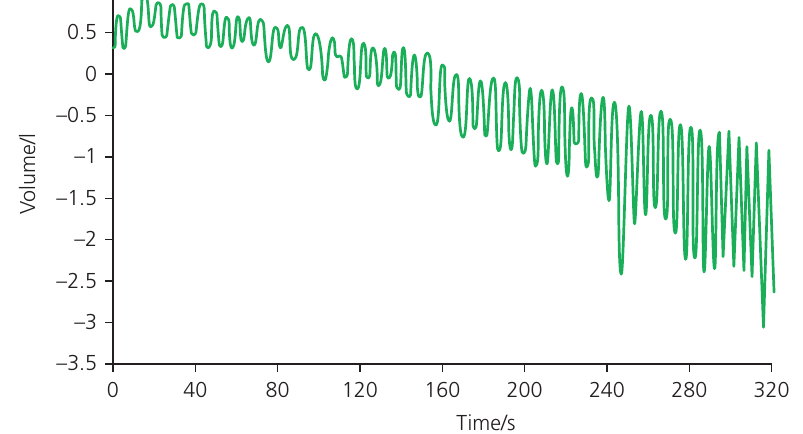
Spirometer traces provide valuable data about breathing patterns. The trace shows volume (vertical axis) changing over time (horizontal axis).
Calculating breathing rate
To find breathing rate, count the number of complete breaths in a known time period, then convert to breaths per minute.
Worked Example: Calculating Breathing Rate from a Spirometer Trace
One breath appears as one complete wave on the trace (the line going up and then down, or down and then up).
Step 1: Count the breaths in a known time period In the trace above, there are breaths in the first seconds ( minutes).
Step 2: Calculate the rate per minute Breathing rate breaths min
Step 3: Verify with another section Between and seconds (another -minute interval), there are approximately - breaths, giving a breathing rate of - breaths min.
Calculating tidal volume
Tidal volume is found by measuring the vertical distance from the peak (top) to the trough (bottom) of a wave. This measurement is more variable than breathing rate because tidal volume naturally fluctuates slightly from breath to breath.
Worked Example: Determining Tidal Volume
In the early part of the trace shown above, tidal volume measures approximately - litres. Later in the recording, it increases to roughly litres, sometimes reaching litres.
Note: Exam mark schemes typically allow more tolerance for tidal volume calculations than for breathing rate.
Understanding trace patterns
All spirometer traces slope downward from left to right. This occurs because:
- The subject re-breathes the same air repeatedly
- The soda lime absorbs carbon dioxide from the air
- However, the subject continues extracting oxygen
- This causes a steady decrease in the total volume of air in the system
- The declining volume creates the downward slope
Additionally, during prolonged spirometry, subjects often begin breathing more deeply and rapidly. This happens because:
- Oxygen concentration in the re-breathed air gradually falls
- Even though is removed, the decreasing level stimulates the body to compensate
- The subject unconsciously takes deeper breaths (increased tidal volume) at a faster rate
- This attempt to obtain more oxygen explains why both measurements increase over time
Safety Consideration
For safety reasons, spirometry experiments should be limited in duration (typically a few minutes) to avoid excessive oxygen depletion.
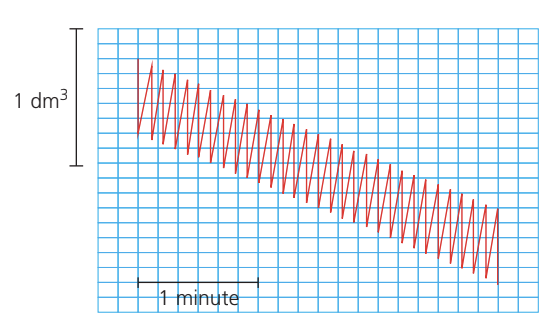
The trace above from a student experiment demonstrates typical patterns. When analyzing such data, look for:
- Regular oscillations indicating individual breaths
- The amplitude (height) of oscillations showing tidal volume
- The frequency of oscillations indicating breathing rate
- The overall downward trend showing oxygen consumption
Key Points to Remember
-
Ventilation maintains concentration gradients essential for gas exchange by constantly refreshing air in the alveoli
-
Inspiration is active: external intercostal muscles and diaphragm contract → thoracic volume increases → pressure decreases → air flows in
-
Normal expiration is passive: muscles relax, lung elasticity causes recoil → thoracic volume decreases → pressure increases → air flows out
-
The respiratory center in the medulla oblongata controls breathing; stretch receptors in the lungs provide negative feedback to regulate the cycle
-
A spirometer measures vital capacity (maximum breath), tidal volume (normal breath at rest), breathing rate (breaths per minute), and oxygen uptake, but cannot measure residual volume