The Heart and Cardiac Activity (OCR A-Level Biology A): Revision Notes
The Heart and Cardiac Activity
Introduction to the mammalian heart
The heart functions as a muscular pump that drives blood circulation throughout the body. Cardiac muscle contracts rhythmically, with the rate of contraction adjustable according to physiological demands. Despite being filled with blood, the heart wall is so thick that it requires its own dedicated blood supply — the coronary circulation — to deliver oxygen and nutrients to the cardiac tissue itself.
The heart's own blood supply is essential because the heart wall is too thick for oxygen to diffuse directly from the blood in the chambers. Without the coronary circulation, the cardiac muscle would quickly become oxygen-starved and unable to function.
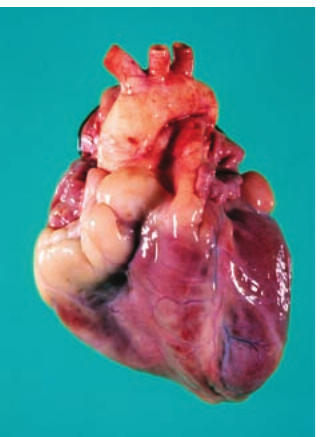
External structure
The aorta emerges from the heart and divides into three main branches. It transports oxygenated blood under high pressure to body tissues. The left ventricle generates this pressure as it contracts and pumps blood into the aorta.
The pulmonary artery carries deoxygenated blood from the right ventricle to the lungs for gas exchange. The coronary artery branches across the heart's surface, supplying the cardiac muscle with oxygenated blood. Blood returns from the heart muscle via the coronary vein. Fatty deposits may accumulate on the heart surface, sometimes obscuring these coronary vessels.
Internal structure of the heart
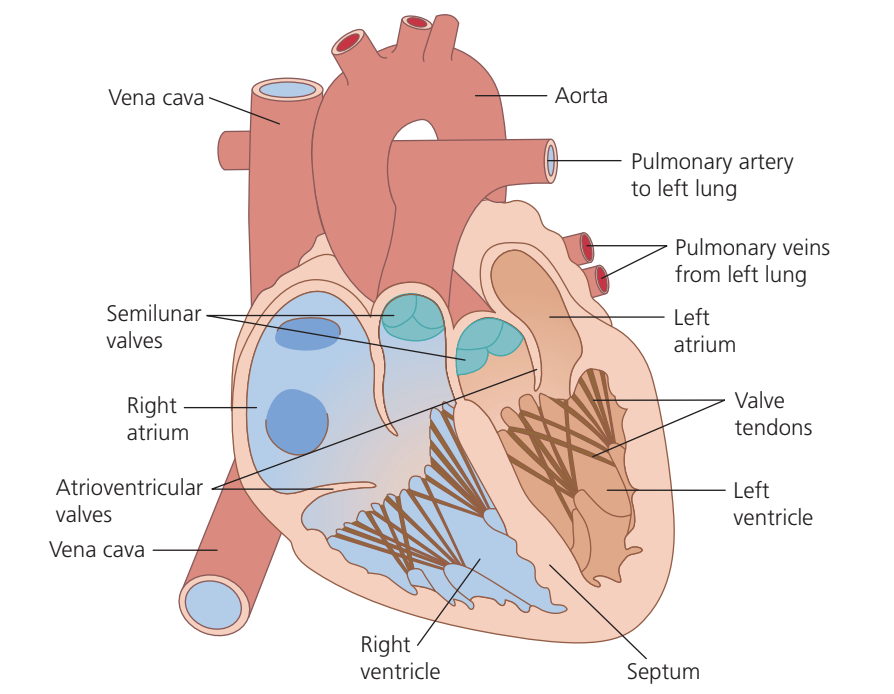
The mammalian heart contains four chambers: two atria (upper chambers) and two ventricles (lower chambers). The heart is divided into right and left halves by the septum, a muscular wall that prevents mixing of oxygenated and deoxygenated blood.
The septum is critical for maintaining separation between oxygenated and deoxygenated blood. Any hole in the septum (a septal defect) would allow blood to mix, reducing the efficiency of oxygen delivery to body tissues.
Blood flow pathway
Worked Example: Complete Blood Flow Pathway Through the Heart
Let's trace the path of a single blood cell through the entire circulatory system:
- Deoxygenated blood enters the right atrium via the vena cava
- Blood flows into the right ventricle
- Right ventricle pumps blood through the pulmonary artery to the lungs
- Gas exchange occurs in the lungs (oxygenation)
- Oxygenated blood returns via the pulmonary veins to the left atrium
- Blood passes into the left ventricle
- Left ventricle pumps blood through the aorta to the entire body (excluding lungs)
- Body tissues extract oxygen, and the cycle repeats
Wall thickness and function
The thickness of each chamber's muscular wall directly relates to its function:
- Left ventricle: Contains the thickest muscular wall because it must generate sufficient pressure to pump blood throughout the entire systemic circulation
- Right ventricle: Has a thinner wall as it only needs to pump blood through the pulmonary circuit to the nearby lungs. The pulmonary circulation offers less resistance because the lungs are spongy, air-filled organs with fewer arterioles and a shorter distance to travel
- Atria: Possess the thinnest walls since they only need to move blood into the adjacent ventricles
The structure-function relationship is clear: greater pumping force required = thicker muscular wall. The left ventricle works against the highest resistance and has the thickest wall, while the atria work against minimal resistance and have the thinnest walls.
Valve systems
Two sets of valves maintain unidirectional blood flow through the heart:
Atrioventricular valves sit between the atria and ventricles. When the ventricles contract, these valves are held in place by valve tendons (chordae tendineae) that attach to the ventricular walls. These tendons prevent the valve flaps from inverting under the considerable pressure generated during ventricular contraction.
Semilunar valves are located at the base of the major arteries leaving the heart (the pulmonary and aortic valves). They prevent backflow of blood into the ventricles after contraction.
Critical Role of Valve Tendons
Without the valve tendons, the atrioventricular valves would be forced backward into the atria during ventricular contraction due to the immense pressure. This would allow blood to flow backward, drastically reducing the heart's pumping efficiency and potentially causing valve damage.
The cardiac cycle
The cardiac cycle describes the sequence of events during one complete heartbeat. The cycle consists of alternating periods of contraction and relaxation. Systole refers to the contraction phase, while diastole describes the relaxation phase.
Pressure changes during the cardiac cycle
Muscular contraction compresses the blood within the heart chambers, increasing blood pressure. By monitoring pressure changes in different heart regions, we can track the cardiac cycle events.
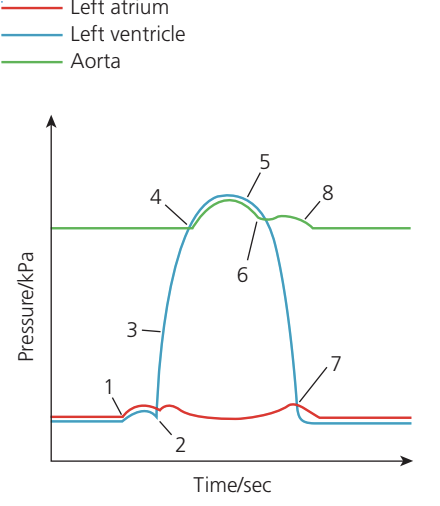
The following sequence describes one cardiac cycle for the left side of the heart (similar events occur on the right):
1. Atrial contraction The atrium contracts, raising pressure slightly due to its relatively thin muscular wall. Blood flows into the ventricle, causing a small pressure increase there.
2. Atrioventricular valve closure As the ventricle begins contracting, ventricular pressure exceeds atrial pressure. This pressure difference forces the atrioventricular valve shut. The atrium relaxes.
3. Ventricular contraction The thick ventricular wall generates substantial pressure as it contracts. The closed atrioventricular valve bulges slightly into the atrium, causing a small rise in atrial pressure.
4. Semilunar valve opening When ventricular pressure surpasses aortic pressure, the semilunar valves open. Blood flows rapidly into the aorta, increasing aortic pressure.
5. Ventricular relaxation begins As the ventricle relaxes, pressure within it decreases.
6. Semilunar valve closure When ventricular pressure drops below aortic pressure, the semilunar valves close, preventing backflow.
7. Atrioventricular valve opening Blood has been accumulating in the atrium, gradually raising atrial pressure. When ventricular pressure falls below atrial pressure, the atrioventricular valve opens and blood flows into the ventricle.
8. Aortic elastic recoil When blood enters the aorta, the elastic arterial walls stretch. As blood flow slows, elastic tissue passively recoils, maintaining blood pressure and flow even when both heart chambers are relaxed. This is passive elastic recoil, not active contraction — the aorta does not "pump" blood.
Understanding Valve Operation
All heart valves open and close passively in response to pressure differences — they do not actively open or close. When pressure is higher behind the valve, it opens; when pressure is higher in front of the valve, it closes. This simple mechanism ensures efficient, one-way blood flow.
Coordination of the heartbeat
Myogenic control
The heart is myogenic, meaning cardiac muscle can initiate its own contractions without requiring external nervous stimulation. The contraction stimulus originates entirely within the heart tissue itself. However, the autonomic nervous system can modify heart rate to match physiological demands. This system controls involuntary functions such as heart rate, blood vessel diameter, and digestion.
The autonomic nervous system has two divisions:
- Parasympathetic nerves: Decrease heart rate
- Sympathetic nerves: Increase heart rate
Myogenic vs Neural Control
Being myogenic means the heart will continue beating even if all nerves to it are severed. In fact, a heart removed from the body and placed in appropriate solution will continue beating! The autonomic nervous system only modulates the rate — it doesn't initiate the heartbeat.
The cardiac conduction pathway
Cardiac contraction follows a precise sequence coordinated by specialised conducting tissue:
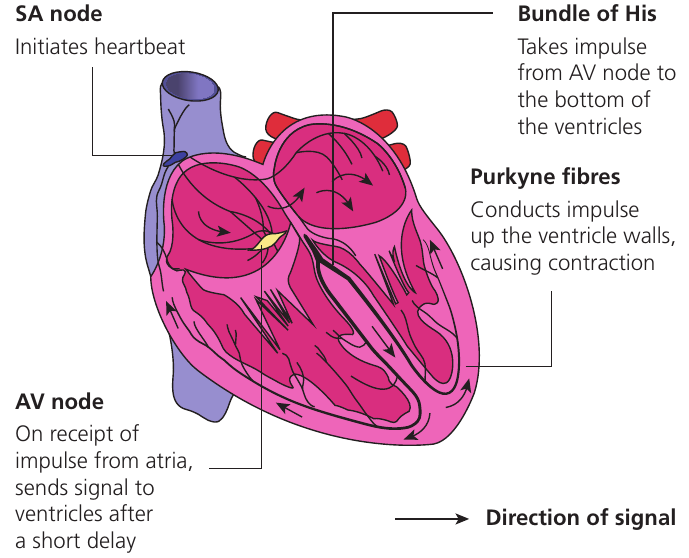
Sino-atrial (SA) node Located in the upper wall of the right atrium, the SA node acts as the heart's natural pacemaker. This specialised tissue generates electrical impulses that trigger a wave of contraction across both atria.
Atrio-ventricular (AV) node Non-conductive tissue separates the atria and ventricles, preventing direct spread of electrical impulses. The AV node provides the only electrical connection between atria and ventricles. It delays the impulse briefly, allowing the atria to complete their contraction before ventricular contraction begins.
Bundle of His After the delay, the AV node transmits the impulse down specialised muscle fibres called the Bundle of His. These fibres conduct the signal rapidly to the bottom of the ventricles.
Purkinje fibres From the base of the ventricles, the impulse travels upward through another set of specialised fibres — the Purkinje fibres (also spelled Purkyne fibres). As the impulse moves up the ventricular walls, it triggers contraction from bottom to top. This ensures blood is efficiently forced upward and out through the arteries at the top of the heart.
Why the AV Node Delay is Essential
The AV node's delay (approximately 0.1 seconds) is crucial for efficient heart function. Without this delay, the atria and ventricles would contract simultaneously, preventing the atria from fully emptying into the ventricles. The delay ensures proper sequential contraction: atria first, then ventricles.
Detecting heart activity
Electrocardiography
Since electrical activity in cardiac muscle drives the heartbeat, this electrical signal can be detected and recorded. Electrocardiography (ECG) involves placing electrodes on the skin to detect electrical signals and produce an electrocardiogram (also abbreviated to ECG).
Normal ECG pattern
A healthy heart produces a characteristic ECG waveform:
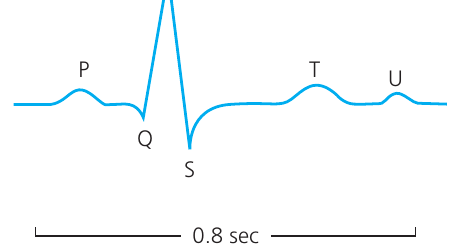
The ECG trace shows several distinctive waves:
- P wave: Results from depolarisation of the atria, causing atrial contraction
- QRS complex: Represents ventricular depolarisation and contraction. The larger amplitude reflects the greater muscle mass of the ventricles
- T wave: Caused by ventricular repolarisation, resulting in ventricular relaxation
- U wave: Origin uncertain
Depolarisation and Repolarisation Explained
Depolarisation refers to the change in electrical charge across cell membranes that triggers muscle contraction. Repolarisation is the restoration of the resting electrical state, allowing muscle relaxation. Think of depolarisation as "switching on" the muscle and repolarisation as "switching off" and resetting for the next contraction.
Heart problems and ECGs
ECG analysis can identify several cardiac rhythm abnormalities:
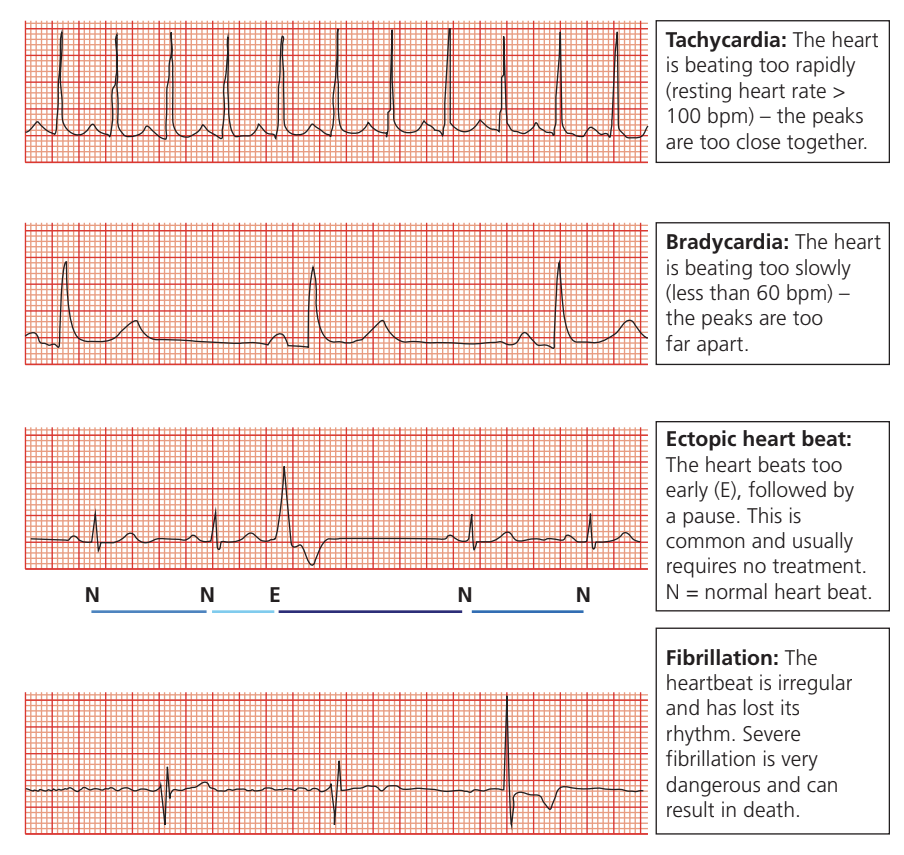
Tachycardia The heart beats excessively rapidly, with a resting heart rate exceeding $100 bpm (beats per minute). On an ECG, the peaks appear too close together.
Bradycardia The heart beats too slowly, with a rate below $60 bpm. ECG peaks are too widely spaced.
While bradycardia is defined as below 60 bpm, trained athletes often have resting heart rates of 40-60 bpm as a normal adaptation to fitness. In these cases, bradycardia is actually a sign of cardiovascular health, not a problem.
Ectopic heartbeat The heart contracts prematurely, followed by a compensatory pause. This common condition usually requires no treatment.
Fibrillation The heartbeat becomes irregular and loses its coordinated rhythm. Severe fibrillation represents a life-threatening emergency that can result in death.
Fibrillation is a Medical Emergency
During fibrillation, the heart muscles contract chaotically instead of in a coordinated manner. This means the heart cannot pump blood effectively, and vital organs (especially the brain) are rapidly deprived of oxygen. Immediate medical intervention with a defibrillator is essential to restore normal rhythm.
Summary
Key Points to Remember:
-
The heart contains four chambers (two atria, two ventricles) with wall thickness matching the force required for their pumping function — the left ventricle has the thickest wall because it pumps blood throughout the entire body
-
The cardiac cycle consists of coordinated atrial and ventricular contraction (systole) and relaxation (diastole), with valve opening and closing determined by pressure differences
-
The heart is myogenic — the SA node initiates each heartbeat, with the signal conducted through the AV node, Bundle of His, and Purkinje fibres to coordinate ventricular contraction from bottom to top
-
ECG traces record the electrical activity of the heart, with the P wave representing atrial depolarisation, the QRS complex showing ventricular depolarisation, and the T wave indicating ventricular repolarisation
-
Abnormal ECG patterns can reveal cardiac problems such as tachycardia (too fast), bradycardia (too slow), or fibrillation (irregular rhythm)