The Eye (HSC SSCE Biology): Revision Notes
The Eye
Introduction to the eye
The eye is a remarkable sensory organ that enables us to perceive the world around us. It contains specialized receptor cells known as photoreceptors, which detect light energy from our surroundings and transform it into electrical nerve impulses. These impulses travel along the optic nerve to the brain, where they are processed and interpreted as the images we see.
Understanding how the eye works involves examining its structure, how it focuses light, the types of receptor cells it contains, and the various disorders that can affect vision. Modern technology also provides several ways to correct vision problems and restore sight.
The process of vision involves three key stages: light detection by photoreceptors, conversion to electrical signals, and interpretation by the brain. This complex system allows us to perceive colors, shapes, movement, and depth in our environment.
Structure and function of the eye
The three layers of the eye
The eye is built from three distinct layers, each with specific roles in vision:
The outer layer (sclera): The sclera forms the tough, protective white coating around most of the eyeball. At the front of the eye, this layer becomes transparent and curved to form the cornea. The cornea plays a crucial role in bending (refracting) incoming light rays as they enter the eye.
The middle layer (choroid): This layer contains the majority of blood vessels that supply the eye with oxygen and nutrients. The rear portion of the choroid is black in colour, which prevents light from scattering inside the eye and ensures images remain sharp. The front section of the choroid forms several important structures: the ciliary body (which controls lens shape), the lens itself, and the coloured iris (which surrounds the pupil).
The inner layer (retina): The retina lines the back two-thirds of the eyeball and is extremely delicate and thin. It contains multiple layers of nerve cells, including the photoreceptor cells (rods and cones) that detect light. These receptors are positioned closest to the back of the eye, where they can receive focused light and convert it into electrical signals.
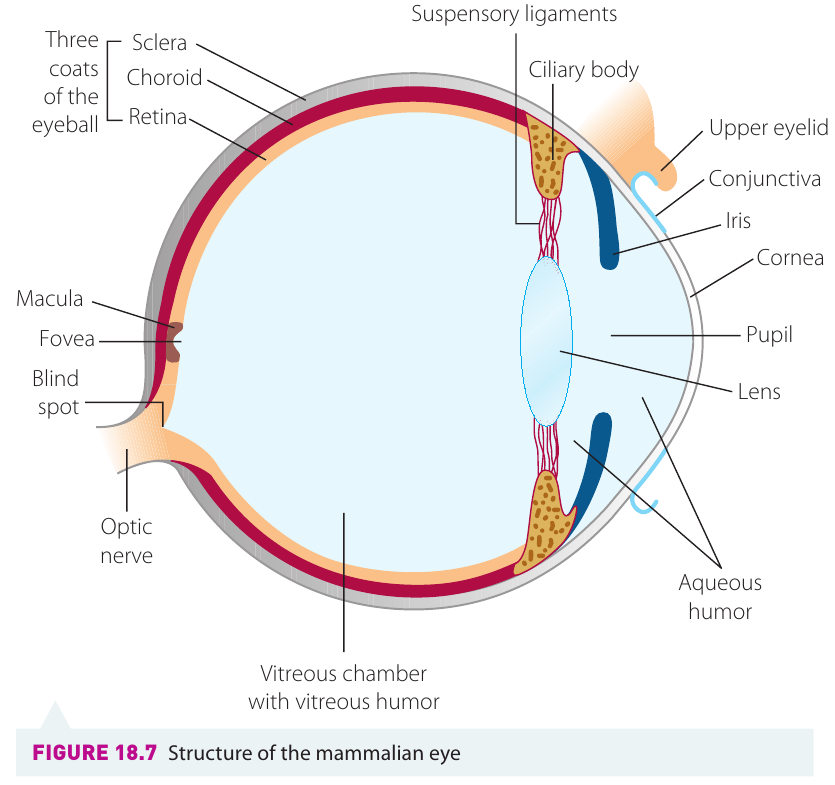
Each layer of the eye has a specialized function: the sclera provides protection, the choroid supplies blood and prevents light scatter, and the retina detects light. All three layers must work together for proper vision to occur.
How light travels through the eye
For us to see clearly, light must pass through several structures within the eye, each of which bends (refracts) the light by a specific amount:
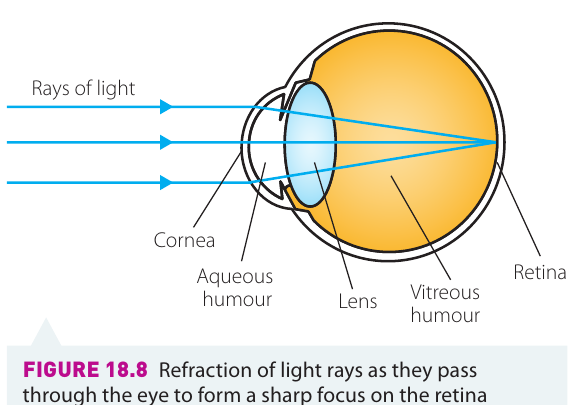
1. Cornea: Light from an object first passes through the curved cornea, which provides most of the eye's refractive power.
2. Aqueous humour: After the cornea, light travels through a clear fluid called aqueous humour (located between the cornea and lens), which provides additional refraction.
3. Pupil: The light then passes through the pupil, which is the dark circular opening in the centre of the eye. The pupil isn't a structure itself—it's simply a hole. The coloured iris (a ring of muscle around the pupil) controls the pupil's size. In bright light, the iris expands to make the pupil smaller, reducing the amount of light entering the eye. In dim light, the opposite occurs, allowing more light to enter.
4. Lens: Next, light passes through the lens, a highly elastic transparent structure with a biconvex (curved outward on both sides) shape. The lens is enclosed in a thin lens capsule and its curvature can be adjusted by the ciliary muscles. This ability to change shape allows the eye to focus on objects at different distances.
5. Vitreous humour: Finally, light travels through the vitreous humour, a jelly-like clear fluid that fills most of the eyeball. This fluid helps refract light slightly and maintains the eye's spherical shape.
6. Retina: The light is focused onto the retina, where photoreceptor cells detect it and generate electrical impulses that are sent to the brain via the optic nerve.
The pathway of light through the eye is: cornea → aqueous humour → pupil → lens → vitreous humour → retina. Each structure contributes to refracting (bending) light rays to ensure they focus precisely on the retina for clear vision.
Special areas of the retina
The fovea: This small depression in the retina is located directly in line with incoming light. The fovea is packed densely with cone cells (but contains no rod cells) and is the region of sharpest vision, called the area of greatest visual acuity. When you look directly at an object, the light from that object falls on your fovea.
The blind spot: At the back of the eye, where nerve fibres converge to form the optic nerve, there are no photoreceptors. Any light falling on this area cannot be detected. However, the brain cleverly fills in the missing information, so we perceive a complete image without noticing this gap.
The fovea provides the sharpest, most detailed vision because of its high concentration of cone cells. This is why you naturally move your eyes to look directly at objects you want to see clearly—you're positioning the image on your fovea.
Accommodation
Accommodation is the process by which the eye adjusts the curvature of the lens to focus on objects at varying distances. This is essential because light from nearby objects needs to be bent more than light from distant objects to form a sharp image on the retina.
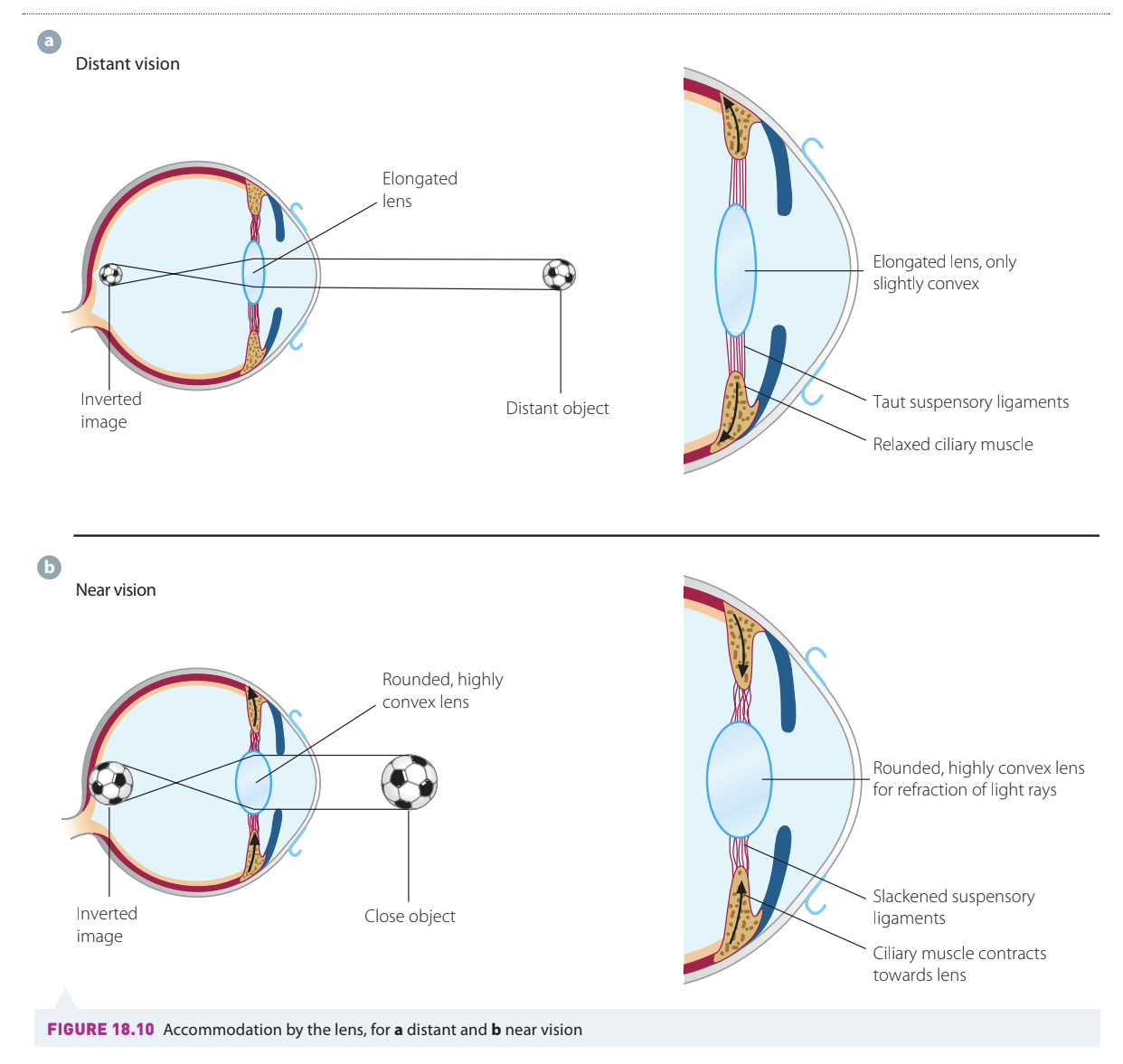
Viewing distant objects
When looking at something far away, the ciliary muscles relax. This pulls the sclera backward, which makes the suspensory ligaments (tiny fibres connecting the ciliary body to the lens) become taut. The tension in these ligaments pulls on the lens, elongating it and reducing its curvature. A flatter lens has less refractive power, which is suitable for distant objects that don't require much additional bending of light rays.
Viewing near objects
When focusing on something close, the ciliary muscles contract and move the sclera forward. This releases tension on the suspensory ligaments, allowing them to slacken. With reduced tension, the naturally elastic lens becomes rounder and more curved. A more curved lens has greater refractive power, bending light rays more sharply to bring the image of the nearby object into focus on the retina.
Worked Example: Accommodation in Action
Imagine reading a book and then looking up to see a bird flying in the distance:
For the book (near object):
- Ciliary muscles contract
- Suspensory ligaments slacken
- Lens becomes rounder (high curvature)
- Greater refractive power bends light rays more
For the bird (distant object):
- Ciliary muscles relax
- Suspensory ligaments become taut
- Lens flattens (low curvature)
- Less refractive power needed
The ability of the lens to change shape in this way depends on its elasticity. As people age, the lens can become less flexible, which may lead to difficulties focusing on close objects (a condition called presbyopia).
Accommodation is an active process for near vision (muscles must contract) but a passive process for distant vision (muscles simply relax). This is why prolonged close work, such as reading or using computers, can cause eye strain—the ciliary muscles must remain contracted for extended periods.
Photoreceptor cells: rods and cones
The retina contains two types of photoreceptor cells: rods and cones. These cells are responsible for detecting light and converting it into electrical signals.
Structure of rods and cones
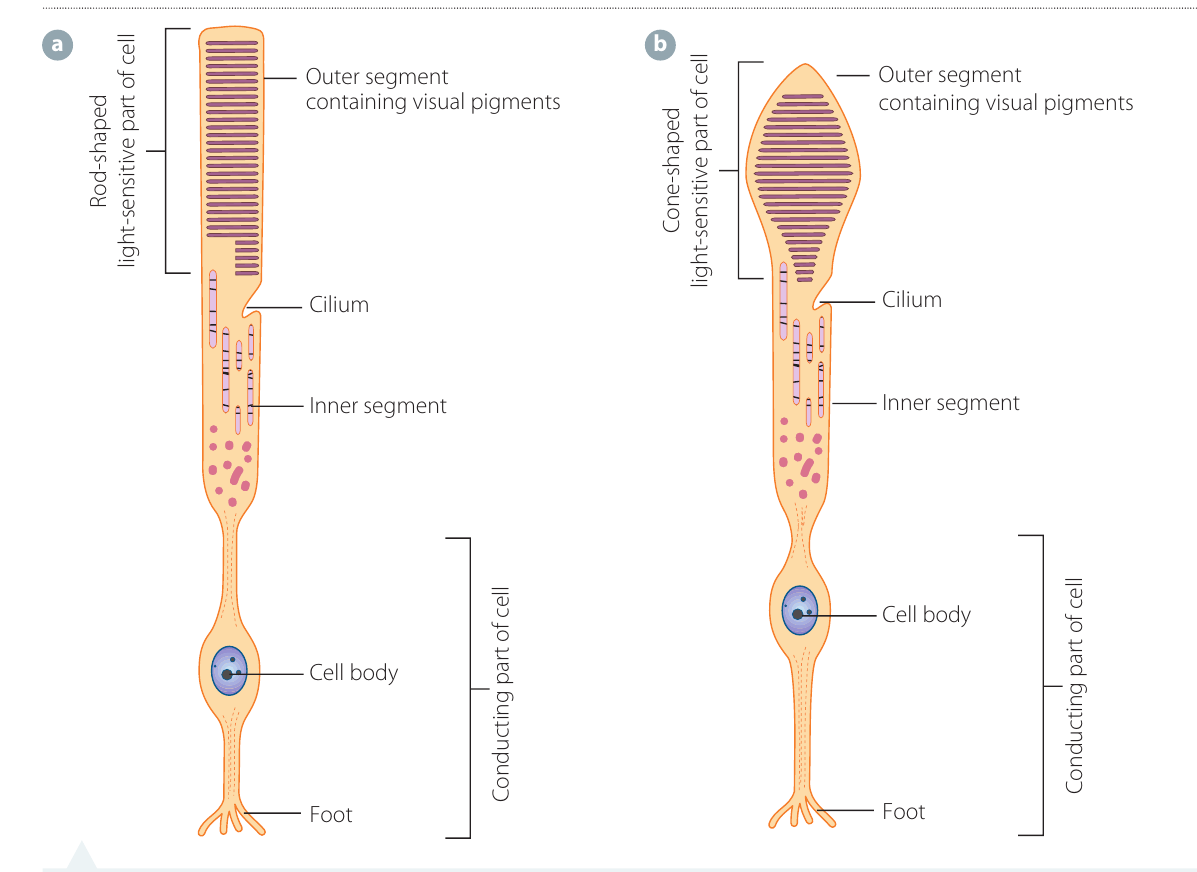
Both rods and cones share a similar basic structure:
- Outer segment: This is the light-sensitive part containing stacks of visual pigment molecules. Rod cells have a long, narrow, cylindrical outer segment, while cone cells have a shorter, wider, cone-shaped outer segment.
- Cilium: A connecting structure between the outer and inner segments.
- Inner segment: Contains cellular machinery and energy-producing structures.
- Cell body: Contains the nucleus.
- Foot: An extension that conducts nerve impulses to the next layer of neurons in the retina.
Distribution in the retina
Rods: The human retina contains approximately 125 million rod cells. They are distributed fairly evenly across most of the retina but are completely absent from the fovea (the central area of sharpest vision).
Cones: Each retina contains about 6-7 million cone cells. They are present throughout the retina but in smaller numbers at the periphery (edges). Cones are most densely concentrated in the fovea.
The different distributions of rods and cones explain why peripheral vision is better in dim light (dominated by rods) while central vision is sharper and color-rich in bright light (dominated by cones in the fovea).
Visual pigments
Both rods and cones contain chemical substances called visual pigments in their outer segments. These pigments absorb light energy and trigger a chemical reaction that generates electrical impulses.
Rhodopsin (in rods): Rod cells contain only one type of visual pigment called rhodopsin. This pigment is extremely sensitive to low levels of light, making rods responsible for night vision and the detection of light and shadow contrasts. Rods also detect movement and provide peripheral vision. However, because they contain only one pigment type, rods cannot distinguish colours.
Iodopsins (in cones): Cone cells contain one of three types of visual pigments called iodopsins. Each type is sensitive to a different wavelength (colour) of light: red, green, or blue. Cones are responsible for colour vision. The brain interprets all the colours we see by combining signals from the three types of cones. Each iodopsin has a peak sensitivity to its particular wavelength but can also detect light at nearby wavelengths, which overlap with other iodopsins. When light of a particular wavelength stimulates multiple cone types, the brain compares the response rates to determine the specific colour.
Key Differences Between Rods and Cones:
- Rods: High sensitivity, function in dim light, detect black and white, no color vision, abundant in periphery
- Cones: Lower sensitivity, require bright light, detect color, provide detailed vision, concentrated in fovea
How visual pigments work
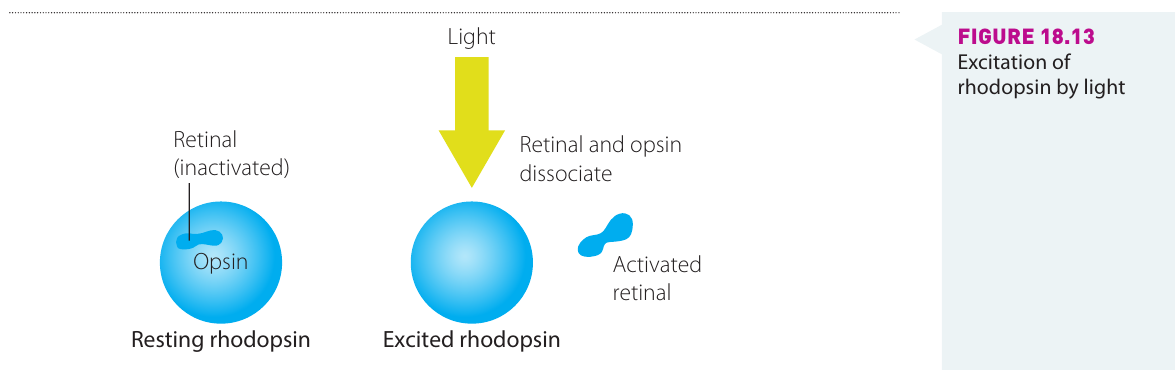
All visual pigments have a similar chemical structure composed of two parts:
- Retinal (also called retinene): A molecule derived from vitamin A.
- Opsin: A protein whose specific type depends on whether the pigment is rhodopsin or one of the iodopsins.
When light strikes a rod or cone cell, it causes the retinal molecule to change shape. This triggers a chemical reaction that transforms light energy into an electrochemical impulse, which travels through the neurons to the brain. At the same time, the retinal and opsin molecules separate (dissociate), and the receptor is temporarily "bleached" and cannot detect more light until the molecules rejoin.
After a period, the retinal and opsin recombine, and the receptor is ready to detect light again. This is why your vision temporarily adapts when moving from bright light to darkness—your visual pigments need time to regenerate.
The dependence of visual pigments on vitamin A explains why vitamin A deficiency can lead to night blindness and other vision problems. A balanced diet containing adequate vitamin A is essential for maintaining healthy vision.
Visual disorders
Several conditions can affect the eye's ability to function properly and produce clear vision.
Myopia (short-sightedness)
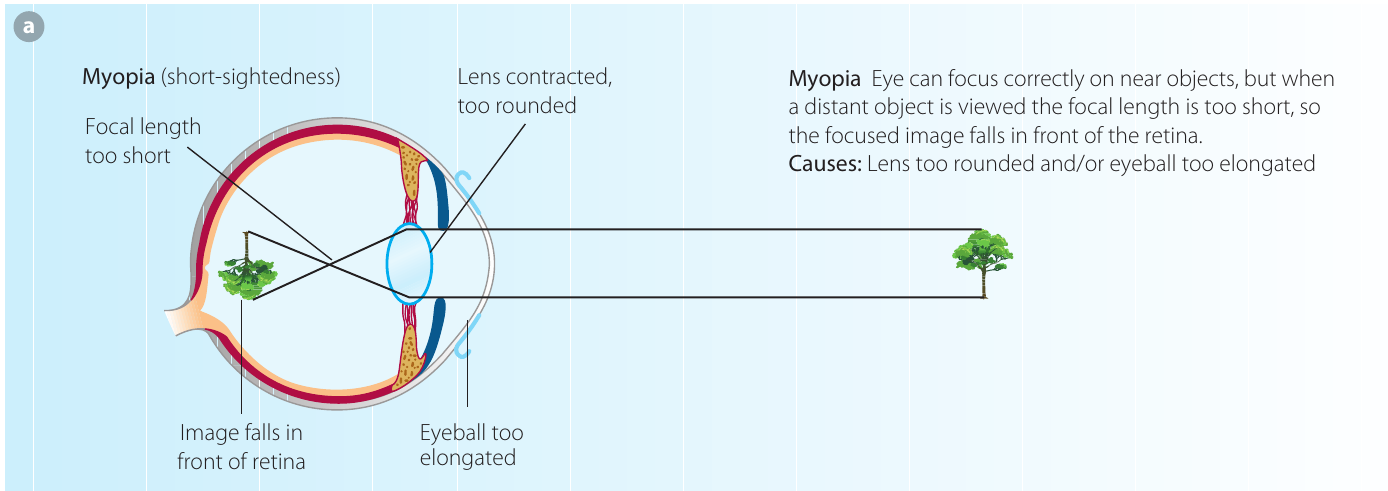
A person with myopia can see nearby objects clearly, but distant objects appear blurred. This occurs because the focused image from a distant object falls in front of the retina instead of on it, while images from near objects focus correctly on the retina.
Causes of myopia:
- The eyeball may be too elongated (too long from front to back)
- The cornea's refractive power may be too strong
- The lens may not flatten sufficiently when the ciliary muscles relax
Myopia is one of the most common vision problems worldwide. It often develops during childhood and adolescence when the eye is still growing. Regular eye examinations can detect myopia early and allow for appropriate correction.
Hyperopia (long-sightedness)
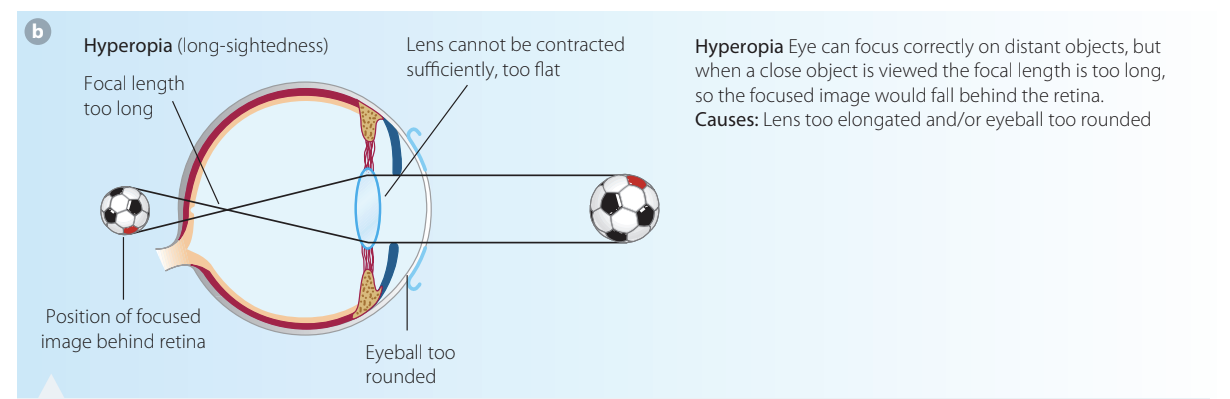
Someone with hyperopia can see distant objects clearly, but near objects are out of focus. This happens because the focused image would theoretically fall behind the retina (though physically it cannot, so the image remains blurred).
Causes of hyperopia:
- The eyeball is too rounded (too short from front to back)
- The lens is too flat and cannot achieve sufficient curvature, often due to loss of elasticity with age
- The cornea's refractive power is inadequate for the eye's shape
Cataracts
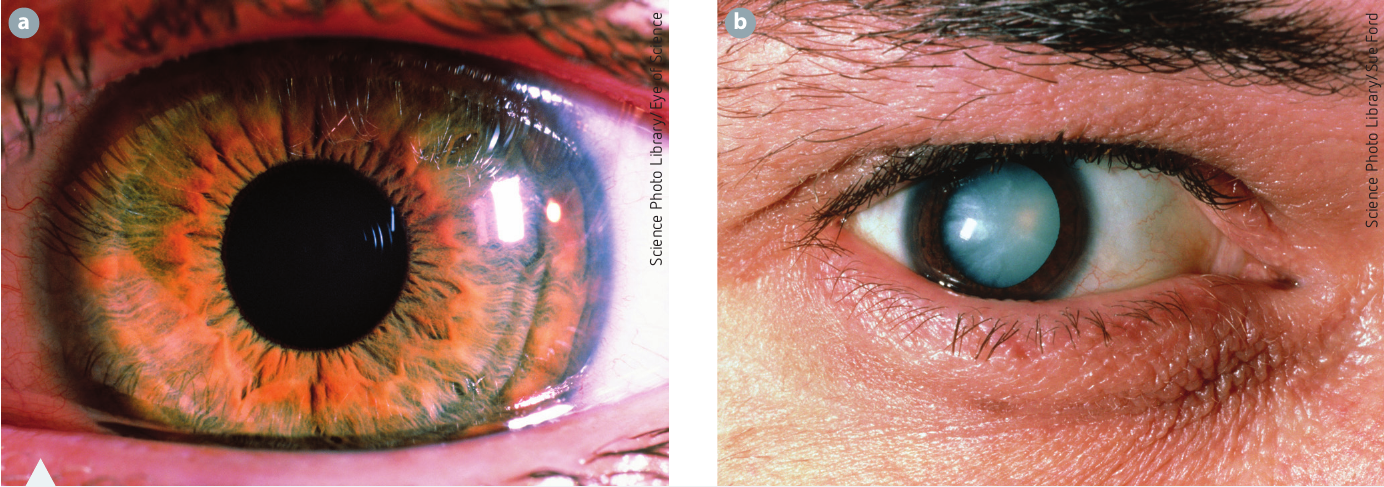
A cataract involves clouding of the lens, which reduces the amount of light that can pass through. This causes blurred vision for both near and distant objects and increased sensitivity to bright sunlight's glare. Cataracts can develop with age or due to other factors such as injury or disease.
Cataracts are a natural part of aging for many people. They develop gradually and can be successfully treated with surgery. Modern cataract surgery has a very high success rate and can significantly improve quality of life.
Macular degeneration
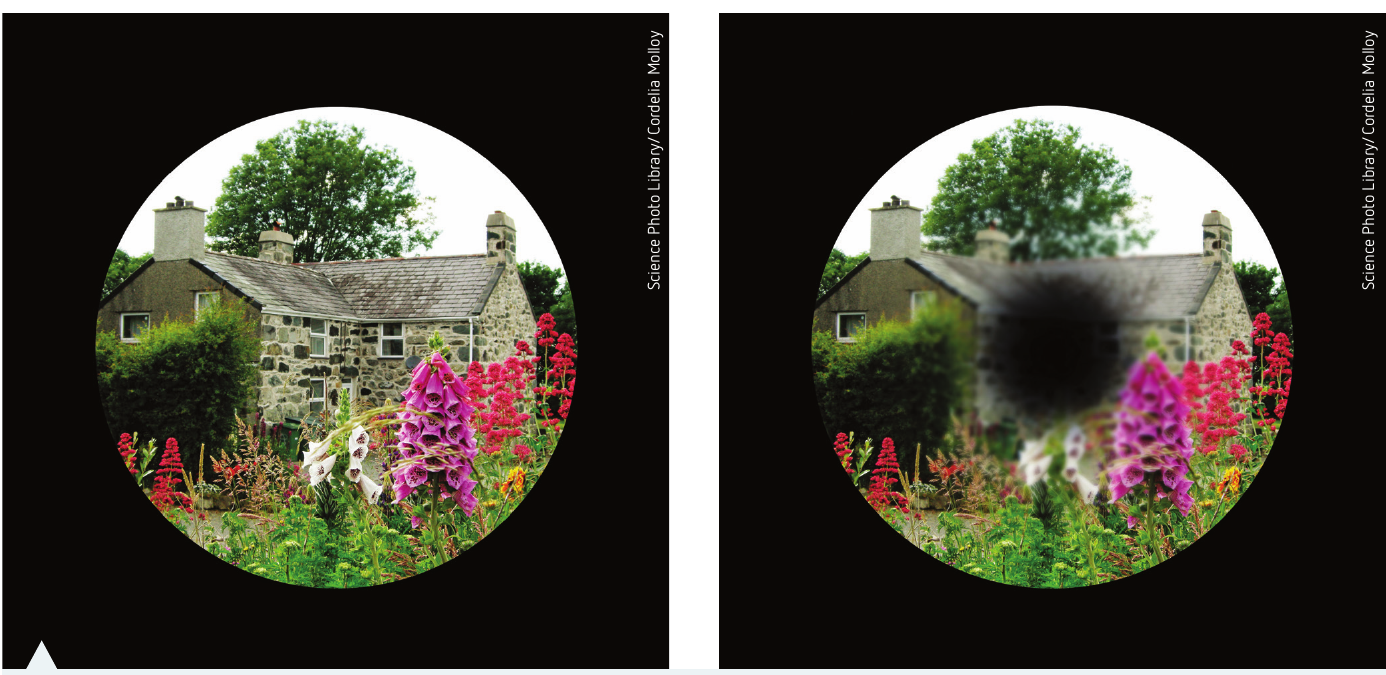
Macular degeneration is a disease affecting the cells beneath the retina, called the retinal pigment epithelium. It is the leading cause of legal blindness in Australia, responsible for 50% of all blindness cases. The disease primarily affects central vision (the area served by the macula and fovea), while peripheral vision remains unaffected. This makes it difficult for affected individuals to read, recognise faces, drive, or perform everyday tasks requiring detailed central vision.
Degeneration of retinal pigment epithelial cells prevents light from being properly focused on this area of the retina. Early detection is crucial for slowing disease progression. Lifestyle changes can reduce risk, including not smoking, maintaining a healthy balanced diet, exercising regularly, and protecting eyes from ultraviolet light.
Risk Reduction for Macular Degeneration:
- Don't smoke
- Maintain a healthy, balanced diet rich in leafy greens and fish
- Exercise regularly
- Protect eyes from UV light with sunglasses
- Have regular eye examinations for early detection
Technologies to assist with visual disorders
Modern technology offers several ways to correct vision problems and help people with visual disorders see more clearly.
Spectacles (glasses)
Spectacles use specially shaped lenses to correct refractive errors in the eye. The lens shape depends on the type of vision problem.
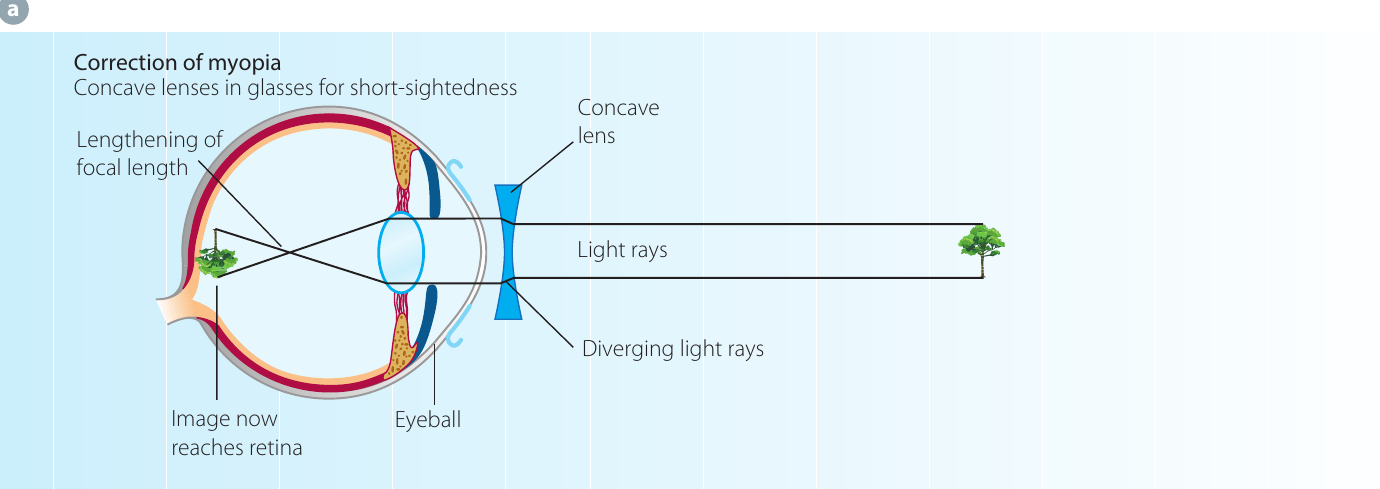
Correcting myopia: Concave lenses (thicker at the edges, thinner in the centre) bend light rays outwards, causing them to diverge before entering the eye. This effectively lengthens the focal length, allowing the image of distant objects to fall on the retina instead of in front of it.
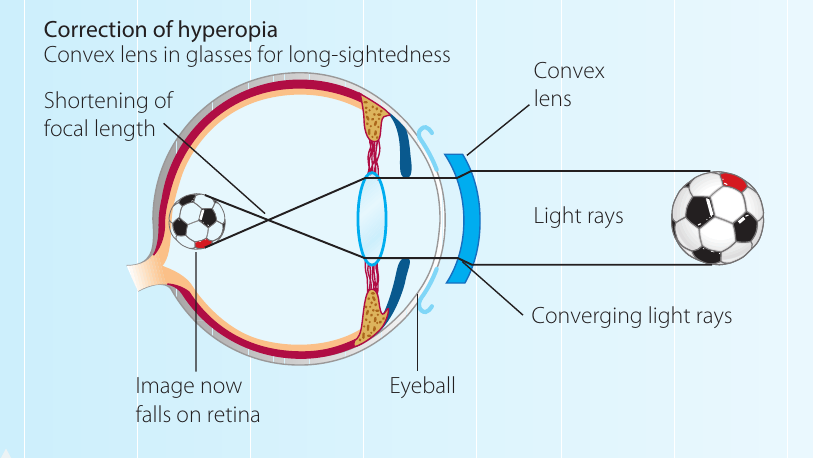
Correcting hyperopia: Convex lenses (thicker in the centre, thinner at the edges) bend light rays inwards, causing them to begin converging before they reach the eye. This shortens the focal length, allowing the focused image of near objects to fall on the retina rather than behind it.
The choice between concave and convex lenses depends on the type of refractive error:
- Myopia (short-sightedness) requires concave lenses to diverge light
- Hyperopia (long-sightedness) requires convex lenses to converge light
Contact lenses
Contact lenses offer an alternative to spectacles for those who prefer not to wear glasses or who are not suitable for laser surgery. They use the same optical principles as spectacles (concave or convex shapes) but are much smaller and shaped to fit the curvature of the eyeball. Contact lenses sit directly on the surface of the eye, providing a wider field of clear vision compared to spectacles.
Laser surgery
Laser surgery (such as LASIK—laser-assisted in situ keratomileusis) is a procedure that changes the curvature of the cornea to correct refractive errors. By reshaping the cornea, surgeons can adjust how light is bent as it enters the eye, allowing it to focus correctly on the retina. This procedure can correct both myopia and hyperopia and may reduce or eliminate the need for spectacles or contact lenses.
LASIK surgery works by using a precise laser to remove microscopic amounts of corneal tissue, permanently altering its shape. The procedure is quick (usually taking less than 30 minutes for both eyes) and most patients experience improved vision within 24 hours.
Cataract surgery
In cataract surgery (intraocular lens implantation or IOL), the cloudy natural lens is removed and replaced with an artificial lens. The surgeon makes a small incision in the eye and uses a device that delivers high-frequency sound waves to break up the clouded lens into small particles. These particles are then suctioned out, and an artificial lens is inserted into the lens capsule. A newer technique uses laser cataract surgery, where a laser breaks up the lens and helps position the artificial lens more accurately.
The bionic eye
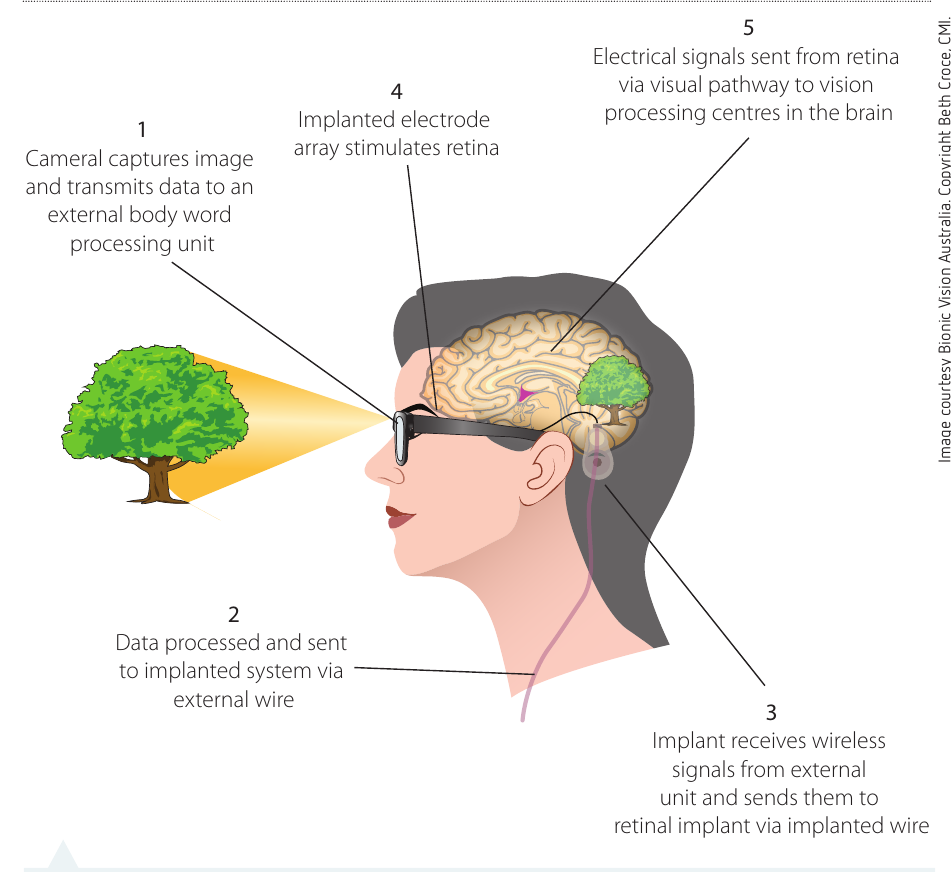
The bionic eye is an emerging technology designed to restore vision to people with conditions like retinitis pigmentosa (where rod and cone cells gradually degenerate) and age-related macular degeneration. The system consists of:
- A camera mounted on glasses that captures images
- A processing unit that converts the images into data
- A microchip implanted in the eye that receives wireless signals
- An electrode array that stimulates the retina's remaining functional cells
- The optic nerve carries these signals to the brain's vision processing centres
The bionic eye bypasses damaged photoreceptors and directly stimulates the cells in the retina that are still functional, allowing some degree of vision to be restored.
While bionic eye technology is still developing and doesn't restore vision to normal levels, it represents a significant breakthrough for people who have lost vision due to retinal diseases. The technology continues to improve, offering hope for better visual restoration in the future.
Remember!
Key Points to Remember:
-
The eye has three layers: the protective sclera (outer), the blood vessel-rich choroid (middle), and the light-detecting retina (inner).
-
Light follows this pathway through the eye: cornea → aqueous humour → pupil → lens → vitreous humour → retina. Each structure refracts (bends) the light to focus it on the retina.
-
Accommodation is the eye's ability to change the lens curvature for near and far vision. For distant objects, ciliary muscles relax and the lens flattens; for near objects, ciliary muscles contract and the lens becomes rounder.
-
Rods detect light in dim conditions and are responsible for night vision and peripheral vision, but cannot see colour. Cones detect colour and provide detailed central vision but require brighter light to function.
-
Common vision problems include myopia (short-sightedness—cannot see distant objects clearly), hyperopia (long-sightedness—cannot see near objects clearly), cataracts (clouded lens), and macular degeneration (damage to central vision).
-
Technologies such as spectacles with concave or convex lenses, contact lenses, laser surgery, cataract surgery, and the bionic eye can correct vision problems or restore sight to people with visual disorders.