Dietary Risks of Low Intake of Fibre and Iron (VCE SSCE Health and Human Development): Revision Notes
Dietary Risks of Low Intake of Fibre and Iron
Understanding how inadequate fibre and iron intake affects Australia's health status and burden of disease is crucial for VCE Health and Human Development students. These dietary risks contribute significantly to chronic diseases and reduced quality of life across the population.
Low intake of fibre
What is fibre?
Fibre is a carbohydrate found in all plant-based foods that is essential for optimal health and wellbeing. Unlike other nutrients, fibre is not absorbed by the body. Instead, it passes through the digestive system, helping you feel full and keeping your digestive tract clean by adding bulk to faeces.

The fact that fibre is not absorbed by the body makes it unique among carbohydrates. This property is what gives fibre its beneficial effects on digestion and feelings of fullness.
Types of fibre
There are two types of fibre, both essential for good health:
Soluble fibre absorbs water to form a gel-like substance. When oats are left in water, they absorb moisture and become mushy. Good sources include:
- Oats
- Fruits and vegetables
- Barley
- Seed husks and flaxseed
- Dried beans, lentils, and peas
- Soy milk and soy products
Insoluble fibre does not absorb moisture and maintains its structure. Fruit and vegetable peels are good examples - they don't change texture in water. Good sources include:
- Wheat bran, corn bran, and rice bran
- Nuts and seeds
- Dried beans
- Wholegrain foods
Memory Tip: Think "Soluble SOAKS water" - soluble fibre absorbs water like oats soaking in milk, while insoluble fibre stays structured like the peel on an apple.
Current consumption patterns
Most Australians consume insufficient fibre. Average daily intake is 20-25 grams, falling short of the Heart Foundation's recommendation of 25-30 grams per day for adults. This gap between actual and recommended intake contributes to several significant health concerns.
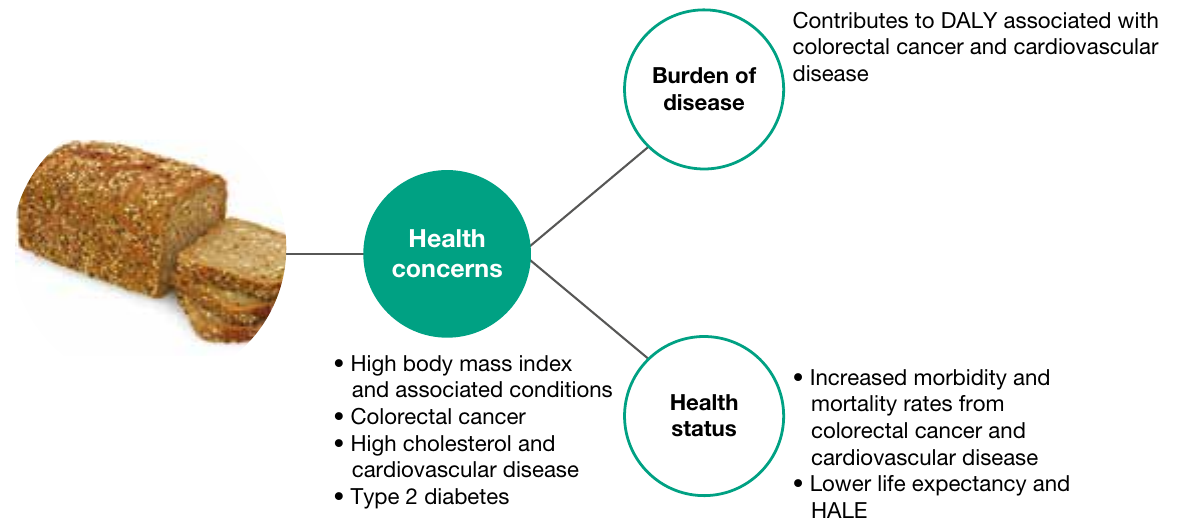
Health impacts of low fibre intake
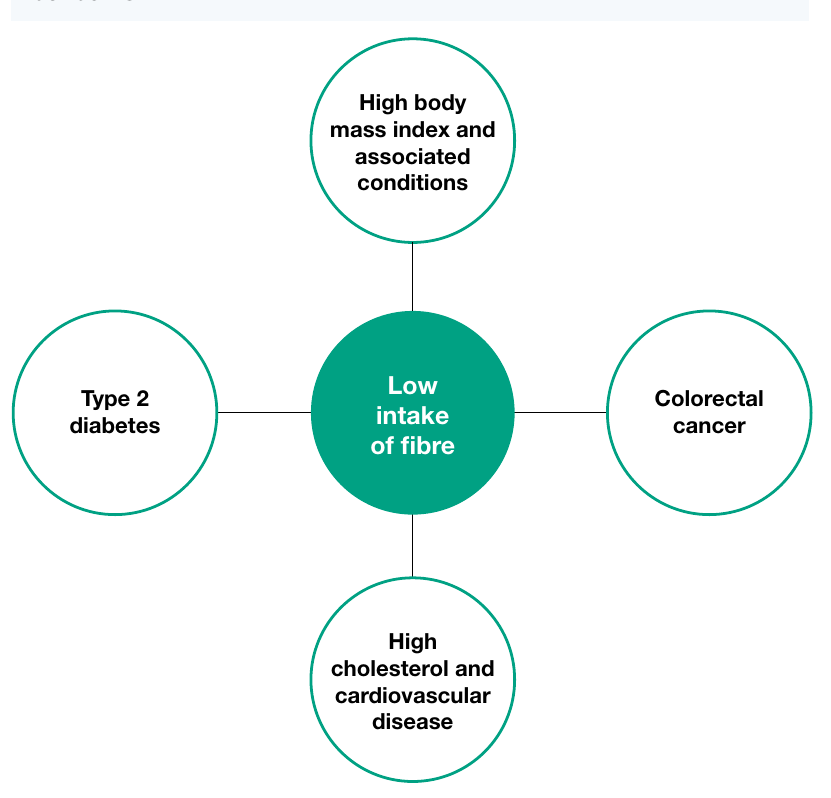
High body mass index
Both types of fibre travel through the digestive system without being absorbed, which promotes feelings of fullness. When fibre intake is low, people may overeat, contributing to high body mass index (BMI).
Soluble fibre absorbs water to form a gel-like substance that slows digestion and delays glucose absorption into the bloodstream. Low soluble fibre intake means more glucose is absorbed by the body, increasing the risk of high BMI and associated conditions such as obesity.
Colorectal cancer
Fibre adds bulk to faeces and helps keep the digestive system clean. This cleaning action reduces the risk of abnormal cells developing, particularly in the colon and rectum. Insufficient fibre intake is associated with higher rates of morbidity and mortality from colorectal cancer, including bowel cancer.

Cardiovascular disease
In the digestive system, soluble fibre attaches to particles of LDL cholesterol and helps remove them from the body. This process decreases cholesterol levels and reduces morbidity and mortality rates from cardiovascular disease. Low fibre intake increases cholesterol absorption and raises the risk of cardiovascular disease.
Understanding the mechanism is crucial: Soluble fibre acts like a "mop" in the digestive system, binding to LDL (bad) cholesterol and removing it before it can be absorbed into the bloodstream. Without adequate soluble fibre, more cholesterol is absorbed, increasing cardiovascular disease risk.
Type 2 diabetes
Research shows that people with low intake of insoluble cereal fibre or wholegrain foods have a significantly higher risk of developing type 2 diabetes. Fibre reduces glucose absorption, which protects against type 2 diabetes by reducing pressure on the pancreas to produce insulin.
Key Connection: Remember the four main health impacts of low fibre intake - Type 2 diabetes, Colorectal cancer, Cardiovascular disease (Cholesterol), and high BMI. All four are linked to how fibre affects digestion and absorption.
Burden of disease from low fibre intake
While the 2015 Australian Burden of Disease Study didn't collect data specifically on low fibre intake, it examined the impact of low intake of wholegrains and high-fibre cereals (both rich sources of fibre).
In 2015, low intake of wholegrains and high-fibre cereals accounted for:
- 1.6% of total disease burden
- 14.1% of burden from coronary heart disease
- 14.0% of burden from type 2 diabetes
- 12.4% of burden from stroke
| Linked disease | DALY Number | Per cent |
|---|---|---|
| Coronary heart disease | 46,452 | 14.1 |
| Stroke | 15,825 | 12.4 |
| Type 2 diabetes | 14,380 | 14.0 |
| Total | 76,657 | 1.6 |
Note: The percentage column shows the proportion of each disease's burden attributable to low wholegrain and high-fibre cereal intake.
Key statistics:
- Fatal burden contributed 72% of overall burden
- Over 83% of stroke burden was due to premature death
- 80% of coronary heart disease burden was due to premature death
- For type 2 diabetes, 68% of burden was non-fatal (YLD rather than YLL)
- Males experienced 65% of the total burden
Exam Focus: Notice that while type 2 diabetes had the highest proportion of non-fatal burden (68%), cardiovascular conditions (stroke and coronary heart disease) were predominantly fatal. This reflects the different nature of these conditions - diabetes is typically chronic and managed, while cardiovascular events are often fatal.
Low intake of iron
Iron's role in the body
Iron is an essential component of blood, forming the 'haem' part of haemoglobin, which carries oxygen throughout the body. Without adequate iron, the body cannot produce enough healthy red blood cells to transport oxygen to cells for energy production.

Red meat is a rich iron source, though it often contains high levels of saturated fat. Therefore, lean cuts should be chosen, and iron should also come from other sources including nuts, brown rice, and eggs. A balanced, varied diet provides the best way to obtain adequate iron.
Iron deficiency anaemia
Insufficient iron intake can lead to iron-deficiency anaemia, characterised by tiredness and weakness. People with this condition struggle to generate enough energy for daily tasks such as school, work, sport, and socialising.
Important Distinction: While various types and causes of anaemia exist, iron deficiency is responsible for 100% of iron-deficiency anaemia cases. Low dietary iron intake is a major cause of iron deficiency, though other causes include inability to absorb iron and severe blood loss.
Key term: Anaemia is a condition characterised by a reduced ability of the body to deliver enough oxygen to cells due to a lack of healthy red blood cells.
Understanding anaemia in depth
How blood cells are produced
Blood cells are constantly produced in bone marrow at a rate of millions per second. Bone marrow is spongy tissue in bone cavities responsible for generating blood's key components, including red blood cells. To create red blood cells, bone marrow requires specific nutrients, including iron, folate, and vitamin B12.
Each red blood cell contains a haemoglobin molecule, which gives red blood cells their colour. When blood reaches the lungs, oxygen molecules attach to haemoglobin and are carried through blood vessels until absorbed by cells.
The Process: Think of haemoglobin as a taxi service for oxygen - it picks up oxygen passengers at the lungs and drops them off at cells throughout the body. Iron is essential for building these "taxis," which is why iron deficiency affects oxygen delivery.
The iron deficiency process
In Australia, iron deficiency is one of the most common causes of anaemia. When dietary iron is insufficient, the body uses stored iron from the liver. Once these reserves are depleted, bone marrow cannot make enough haemoglobin, potentially resulting in anaemia.
Anaemia occurs when there is a reduced level of red blood cells or haemoglobin in the blood. The heart then pumps harder to ensure adequate oxygen delivery to cells. During exercise, meeting cellular oxygen demands becomes increasingly difficult, leading to exhaustion.
Who is at risk?
Certain groups face higher anaemia risk:
- Females: Particularly susceptible due to menstruation and pregnancy. Estimates suggest around one in five menstruating females and half of all pregnant females are anaemic
- Youth during puberty: Blood volume increases during puberty, raising demand for red blood cells and haemoglobin
Critical Understanding: Females face significantly higher risk due to blood loss during menstruation and increased iron demands during pregnancy. This explains why the burden of disease statistics show such a striking gender disparity.
Causes of anaemia
Anaemia results from a malfunction in the body rather than being a disease itself. While commonly associated with deficiencies in iron, folate, and/or vitamin B12, anaemia can also result from:
- Malabsorption: Occurs when consumed nutrients cannot be used, caused by conditions such as coeliac disease
- Inherited disorders: Blood disorders like thalassaemia and sickle cell disease can be inherited from parents
- Chronic conditions: Conditions such as rheumatoid arthritis and tuberculosis can contribute
- Bone marrow conditions: Including cancer or infection
- Blood loss: Due to injury, surgery, cancer, stomach ulcers, heavy periods, or frequent blood donation
- Rapid growth periods: During puberty or pregnancy when large amounts of energy are required
Don't Assume: A common misconception is that anaemia is always caused by low dietary iron intake. As this list shows, anaemia has multiple causes, some of which cannot be prevented through diet alone. Treatment must address the underlying cause.
Symptoms of anaemia
Depending on severity, anaemia symptoms can include:
- Pale skin
- Tiredness and weakness
- Shortness of breath
- Blood pressure drops when standing suddenly (sometimes from blood loss during heavy menstrual periods)
- Headaches
- Fast pulse
- Irritability
- Difficulty concentrating
- Cracks or redness of the tongue
- Appetite loss
- Strange food cravings, including desire to eat dirt or rice (a condition called pica)
Memory Aid - "SWEPT": Key symptoms to remember are Shortness of breath, Weakness, Exhaustion, Pale skin, and Tiredness. These reflect the body's struggle to deliver adequate oxygen to cells.
Treatment and prevention
Treatment
Treatment depends on severity and cause. The underlying cause must be addressed alongside symptoms.
- Vitamin and mineral supplements may be needed for dietary deficiency
- Iron injections may be required if iron levels are particularly low
- Iron supplements should only be used under medical direction, as the body doesn't excrete iron efficiently, which can lead to iron poisoning if dosage isn't monitored
Warning: Never self-prescribe iron supplements. The body cannot efficiently remove excess iron, which can accumulate to toxic levels. Always consult a healthcare professional before taking iron supplements.
Prevention
Anaemia caused by dietary deficiencies can be prevented by regularly consuming:
- Lean meats
- Nuts and legumes
- Fruit and vegetables
- Dairy products
- For vegans: Fortified foods or vitamin and mineral supplements may be necessary
Anaemia caused by underlying health conditions may not be preventable as it results from faults in the cell-making process, though treatments can relieve symptoms.
Burden of disease from low iron intake
In 2015, iron deficiency contributed over 17,000 years of healthy life lost (DALY). The burden fell predominantly on females under 45 years of age.
Impact on females:
- Ages 0-14: Iron deficiency was the second largest cause of disease burden (1% of total burden)
- Ages 15-24: Sixth leading cause (1.6% of total burden)
- Ages 25-44: Tenth leading cause (1.5% of total burden)
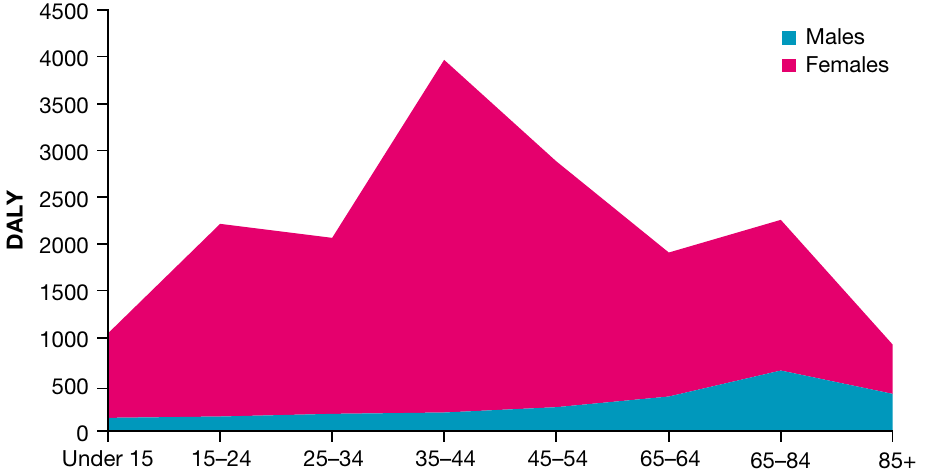
Key statistics:
- 99.1% of burden was due to non-fatal outcomes (YLD)
- 86% of total burden was experienced by females
- Peak burden occurred in the 35-44 age group for females
- Males experienced minimal burden across all age groups
Exam Tip: When discussing burden of disease from iron deficiency, always note the striking gender disparity and age distribution. Females of reproductive age are disproportionately affected, which relates to menstruation and pregnancy demands. The 99.1% non-fatal burden indicates iron deficiency causes significant disability but rarely results in death.
Remember!
Key Points to Remember:
-
Fibre is essential: Two types (soluble and insoluble) have different properties but both are crucial for health. Most Australians consume only 20-25g daily versus the recommended 25-30g. Soluble fibre absorbs water and helps remove cholesterol; insoluble fibre adds bulk and keeps the digestive system clean.
-
Low fibre contributes to multiple diseases: Including high BMI, colorectal cancer, cardiovascular disease, and type 2 diabetes. It accounted for 1.6% of total disease burden in 2015, with males experiencing 65% of this burden. The mechanism involves reduced feelings of fullness, increased glucose absorption, higher cholesterol levels, and inadequate digestive system cleaning.
-
Iron is vital for oxygen transport: Iron forms part of haemoglobin in red blood cells, which carry oxygen throughout the body. Inadequate iron leads to anaemia, characterised by tiredness and weakness. The body requires iron, folate, and vitamin B12 to produce healthy red blood cells in bone marrow.
-
Anaemia has multiple causes: While dietary iron deficiency is common, anaemia can also result from malabsorption, inherited disorders, chronic conditions, bone marrow problems, blood loss, and rapid growth periods. Treatment must address the underlying cause, not just symptoms.
-
Anaemia disproportionately affects females: 86% of iron deficiency burden falls on females, particularly those under 45 years due to menstruation and pregnancy. Peak burden occurs in the 35-44 age group. 99.1% of burden is non-fatal (YLD), indicating significant disability without high mortality.
-
Prevention is possible: Both fibre and iron deficiencies can be prevented through balanced, varied diets including wholegrains, fruits, vegetables, lean meats, nuts, and legumes. However, prevention focuses on dietary causes - some forms of anaemia resulting from underlying health conditions may not be preventable through diet alone.