The Kidney (OCR A-Level Biology A): Revision Notes
The Kidney
Overview of kidney function
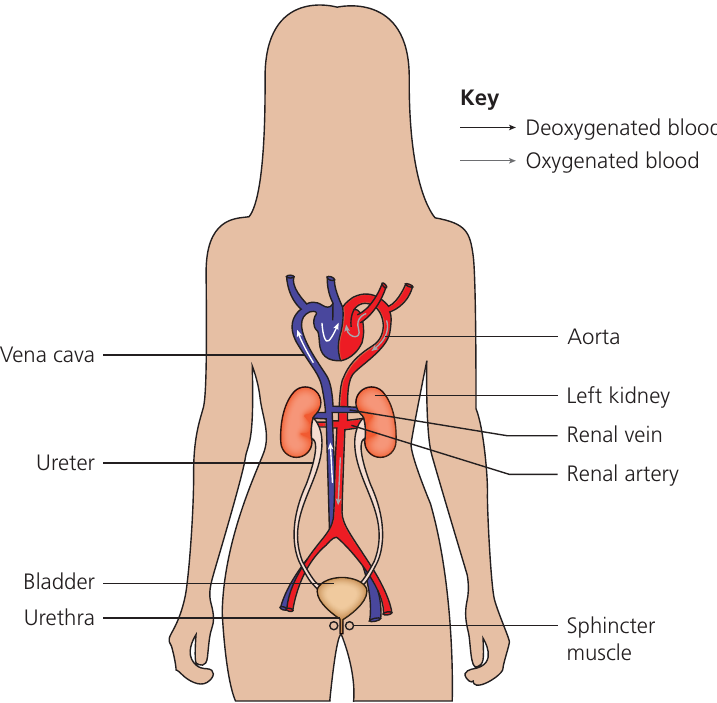
Kidneys are located in the upper abdomen, just below the diaphragm, and serve as the body's primary excretory organs. These organs perform several vital homeostatic functions:
- Filtering blood to remove metabolic waste products (particularly urea)
- Regulating water balance in the body
- Controlling concentrations of major ions including , , , , , and phosphate
- Maintaining blood pH
- Preventing harmful accumulation of excretory products
The kidneys continuously filter blood to maintain these substances at safe, constant concentrations. When protein intake increases beyond what is needed for growth and repair, excess amino acids are converted to urea, which must be efficiently removed to prevent toxicity.
The kidneys process approximately 180 litres of filtrate per day, yet only produce 1-2 litres of urine. This demonstrates the remarkable efficiency of the reabsorption processes occurring in the nephrons.
Gross structure of the kidney
The kidney exhibits distinct structural regions visible to the naked eye:
External features
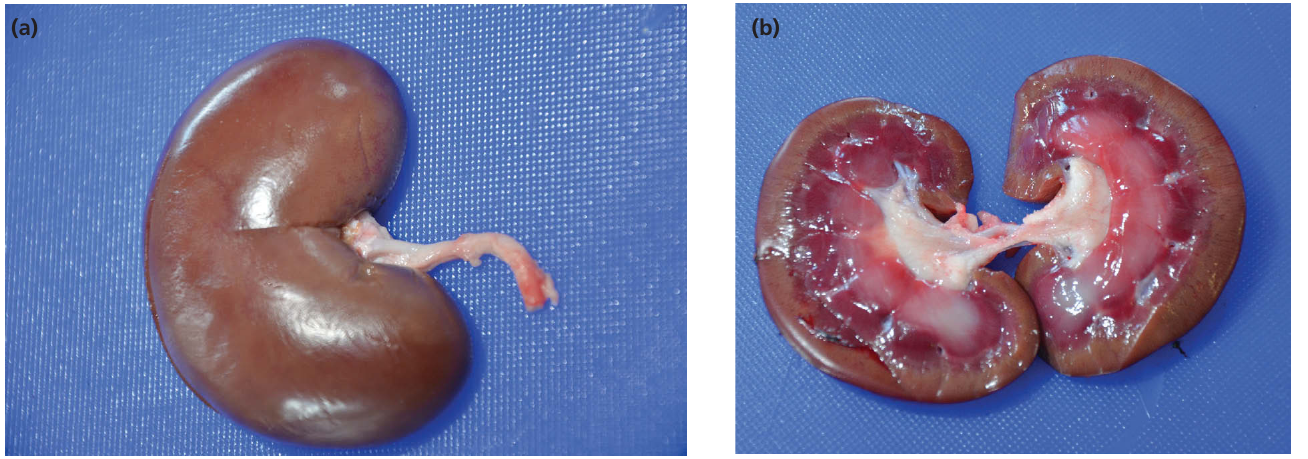
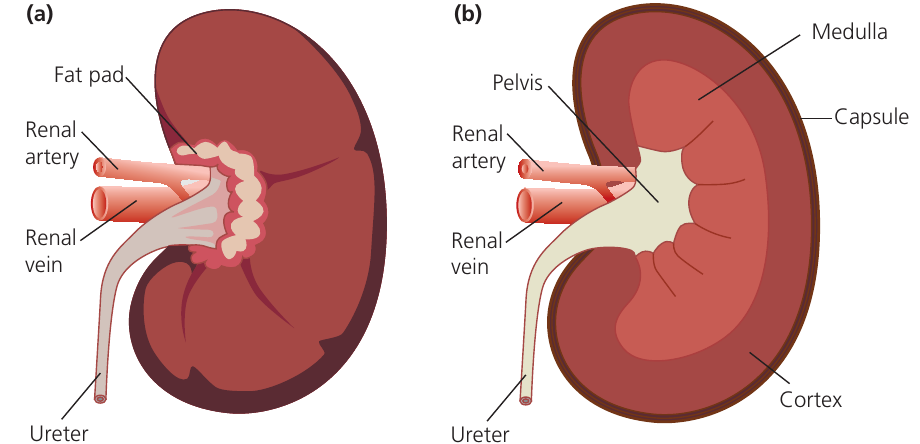
The kidney is a bean-shaped organ protected by a thin capsule of connective tissue containing collagen fibres. Blood enters via the renal artery and exits through the renal vein. The ureter carries urine away from the kidney to the bladder. A fat pad surrounds the kidney providing protection and insulation.
Internal anatomy
When sectioned vertically, three main regions become visible:
Cortex (outer region): Contains the glomeruli, proximal convoluted tubules (PCT), and distal convoluted tubules (DCT), along with numerous blood vessels. This is where ultrafiltration and selective reabsorption occur.
Medulla (middle region): Composed of loops of Henle and collecting ducts, surrounded by associated capillaries called vasa recta. The medulla creates a concentration gradient essential for water reabsorption.
Pelvis (inner region): A urine-filled space lined with white fibrous tissue that connects to the ureter. This region collects urine from the collecting ducts before it passes to the bladder.
The distinct layering of the kidney (cortex, medulla, pelvis) reflects the functional organization of nephrons. Each region performs specific roles in the overall process of blood filtration and urine formation.
The nephron - functional unit of the kidney
A nephron is the functional unit of the kidney that filters blood, reabsorbs useful substances, and forms urine. Each nephron consists of a glomerulus, a tubule system, and associated blood capillaries. At birth, each kidney contains approximately one million nephrons, though this number decreases with age.
Structure of a complete nephron
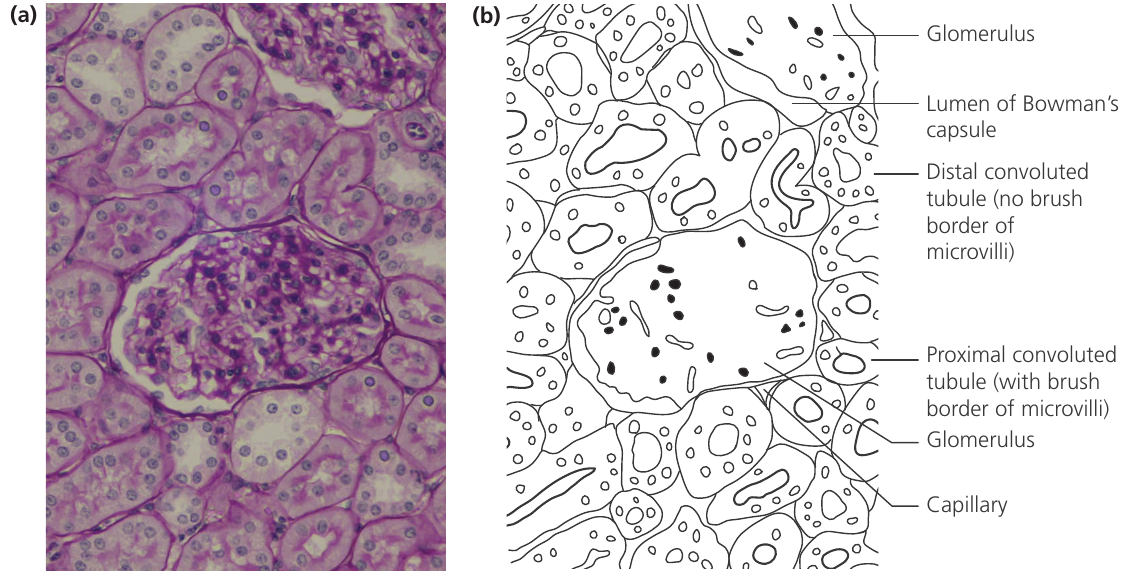
Nephrons are not visible as complete structures in tissue sections because they do not lie in a single plane. Microscope sections reveal parts of many adjacent nephrons rather than one complete unit.
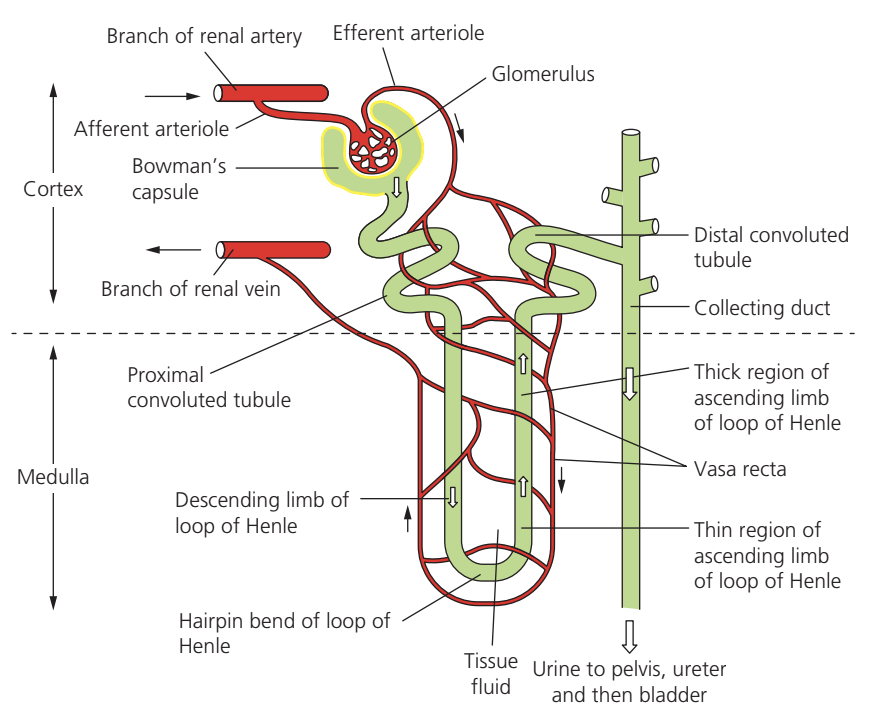
The nephron comprises several distinct regions, each with specialised structure and function:
Bowman's capsule: A cup-like structure surrounding the glomerulus. It is lined by a single layer of squamous epithelial cells and collects the filtrate formed during ultrafiltration.
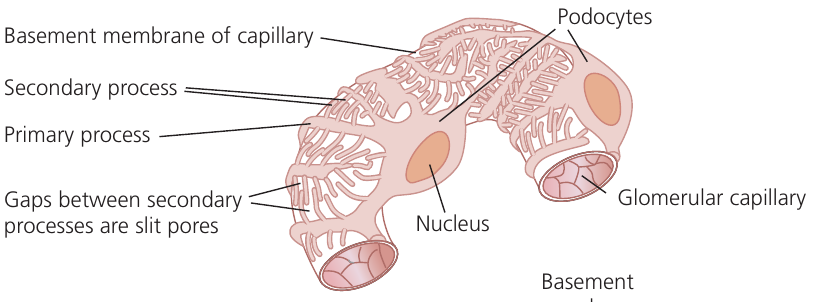
Glomerulus: A tightly coiled network of capillaries suspended within Bowman's capsule by specialised cells called podocytes (literally "foot cells"). These cells have branching extensions with prominent nuclei visible in microscope sections.
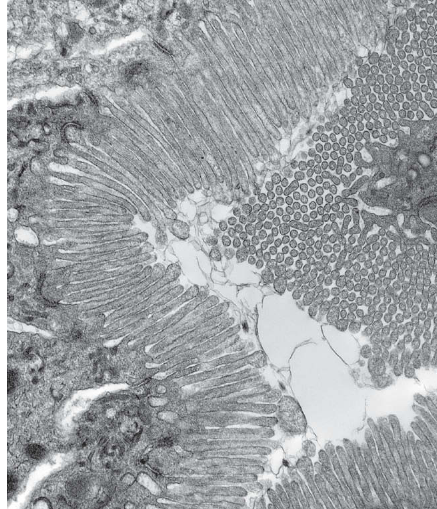
Proximal convoluted tubule (PCT): Formed from cuboidal epithelial cells featuring a prominent brush border of microvilli on the luminal surface. These cells contain numerous mitochondria to power active transport processes. The PCT is wider in cross-section than other tubule regions.
Loop of Henle: Comprises a descending limb, hairpin bend, and ascending limb. The descending limb extends into the medulla with a squamous epithelium. The ascending limb returns toward the cortex and has two regions: a thin region near the hairpin with squamous epithelium, and a thick region with cuboidal epithelial cells rich in mitochondria but lacking a brush border.
Distal convoluted tubule (DCT): Located in the cortex with cuboidal cells narrower than those of the PCT. These cells have few microvilli and no brush border, distinguishing them from PCT cells in microscope sections.
Collecting duct: Wider in cross-section than other nephron parts. Multiple nephrons drain into each collecting duct. The epithelium is cuboidal without a brush border, similar to DCT cells. These ducts extend through the medulla to the pelvis.
The different epithelial cell types found in each region of the nephron reflect their specific functions. For example, the brush border in PCT cells provides massive surface area for reabsorption, while the mitochondria-rich cells in the thick ascending limb support the energy-demanding active transport processes.
Ultrafiltration in the glomerulus
Blood enters the glomerulus from a branch of the renal artery under high pressure. This pressure is maintained because the efferent arteriole (carrying blood away) has a narrower diameter than the afferent arteriole (bringing blood in), creating a "head" of pressure.
Ultrafiltration is an enhanced form of pressure filtration with specialised structural adaptations that make it highly efficient at removing substances from blood. The process is driven by the net effect of four pressures:
- Hydrostatic pressure of blood (forces fluid out)
- Oncotic pressure of blood plasma proteins (opposes filtration)
- Hydrostatic pressure of filtrate (opposes filtration)
- Oncotic pressure of filtrate (negligible effect)
The difference in diameter between afferent and efferent arterioles is crucial - this creates the high hydrostatic pressure needed to force fluid through the filtration barrier. Without this pressure difference, ultrafiltration would not occur efficiently.
Structural adaptations for ultrafiltration
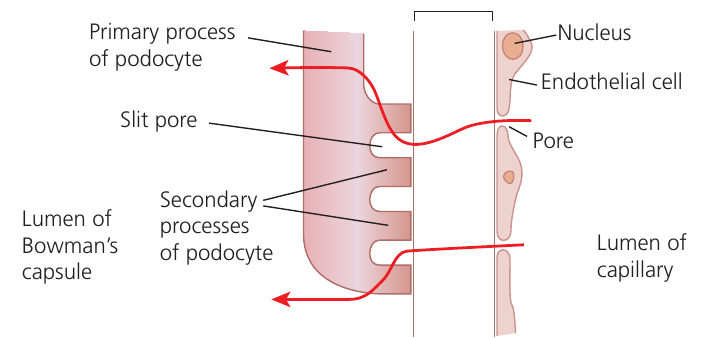
The glomerular filtration barrier consists of three layers that determine what can pass into the filtrate:
Fenestrated endothelium: The capillary walls contain numerous pores that allow substances to leave the blood freely while retaining blood cells and platelets.
Basement membrane: A layer of glycoproteins acting as a molecular sieve. It retains blood cells, platelets, and most plasma proteins (those with relative molecular mass above ). Smaller molecules including water, glucose, amino acids, urea, and small ions pass through freely.
Podocyte layer: These specialised cells have primary processes extending from the cell body, which branch into secondary processes (pedicels or "foot processes"). These interdigitate to create filtration slits (slit pores) between them. This incomplete layer offers minimal resistance to filtrate flow while supporting the capillaries.
The combination of high blood pressure and these structural adaptations produces approximately of filtrate (the glomerular filtration rate, GFR) in healthy individuals.
The three-layered filtration barrier is remarkably selective - it allows small molecules to pass while retaining all blood cells and most proteins. Any damage to this barrier (e.g., in kidney disease) can result in protein or blood appearing in urine, indicating compromised kidney function.
Selective reabsorption in the proximal convoluted tubule
The filtrate collecting in Bowman's capsule contains both waste products and valuable substances that must be recovered. The PCT cells are highly specialised for reabsorbing:
- Glucose
- Amino acids
- Sodium ions and other minerals
- Water
Mechanism of glucose reabsorption
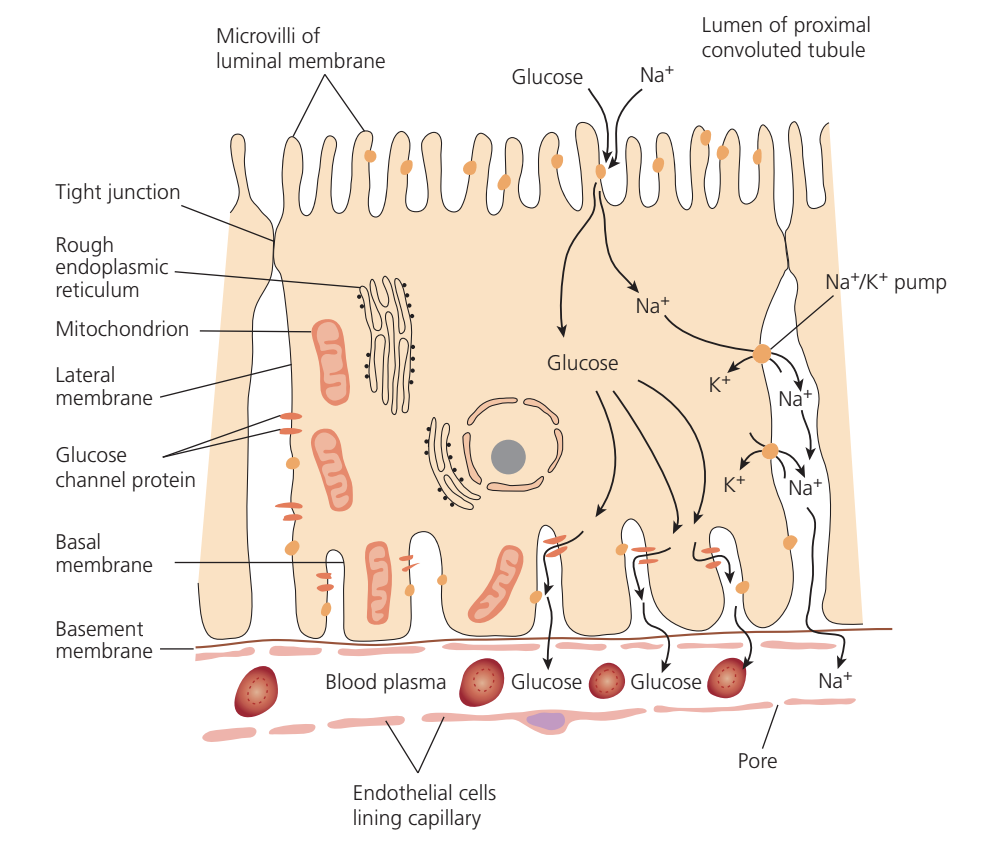
Reabsorption of glucose and amino acids requires ATP, making this an active process with an indirect mechanism:
- pumps in the basal and lateral membranes actively transport sodium out of the cell into tissue fluid, using ATP from mitochondria
- This creates a low sodium concentration inside the cell, establishing a concentration gradient from the filtrate into the cytoplasm
- On the luminal membrane facing the filtrate, symport (co-transporter) proteins have binding sites for both sodium ions and glucose
- When both sites are occupied, the carrier protein changes shape, delivering both sodium and glucose into the cytoplasm
- Glucose concentration builds up inside the cell and glucose diffuses out through facilitated diffusion carriers in the basal membrane into blood capillaries
This process is called indirect active transport because glucose itself moves by diffusion, but this movement depends on the active transport of sodium ions. Similar mechanisms reabsorb amino acids.
Worked Example: How Indirect Active Transport Works
Think of the sodium-potassium pump as creating a "pulling force":
Step 1: The pump uses ATP to actively transport out of the cell
- This creates LOW concentration inside the cell
- This creates HIGH concentration in the filtrate
Step 2: Sodium "wants" to flow back into the cell down its concentration gradient
- Symport proteins use this "pull" to bring glucose along
- Like hitchhiking - glucose gets a free ride with sodium
Step 3: The result
- Glucose is moved into the cell without direct ATP use
- But it only works because ATP was used to pump out sodium first
- Hence "indirect" active transport
Passive reabsorption
Some substances move without direct energy input:
- Urea diffuses across PCT cells back into the bloodstream following its concentration gradient
- Water moves by osmosis from the filtrate to blood because solute reabsorption creates a water potential gradient
Structure-function relationships in PCT cells
PCT cells demonstrate excellent correlation between structure and function:
- Tight junctions between cells (like Velcro) ensure substances move through cells rather than between them, maintaining control over reabsorption
- Microvilli create a brush border providing extensive surface area for symport carrier proteins
- Numerous mitochondria supply ATP for pumps through aerobic respiration
- Infolded basal membrane increases surface area for protein pumps and glucose carrier proteins
- Rough endoplasmic reticulum synthesises carrier proteins, symport proteins, and pump proteins
By the end of the PCT, approximately 99% of the filtrate volume has been reabsorbed, with the remaining fluid passing into the loop of Henle.
The impressive efficiency of PCT reabsorption means that of the 180 litres of filtrate produced daily, around 178 litres are recovered here. This prevents massive fluid loss and conserves valuable nutrients like glucose and amino acids.
Creating a water potential gradient - the loop of Henle
Mammals possess two types of nephron: those with short loops barely entering the medulla, and those with long loops extending to the medulla's tip. Human kidneys contain approximately short loops and long loops.
The loop of Henle's primary function is to create tissue fluid in the medulla with very low water potential. This concentrated tissue fluid is essential for water reabsorption from urine in the collecting ducts when the body needs to conserve water.
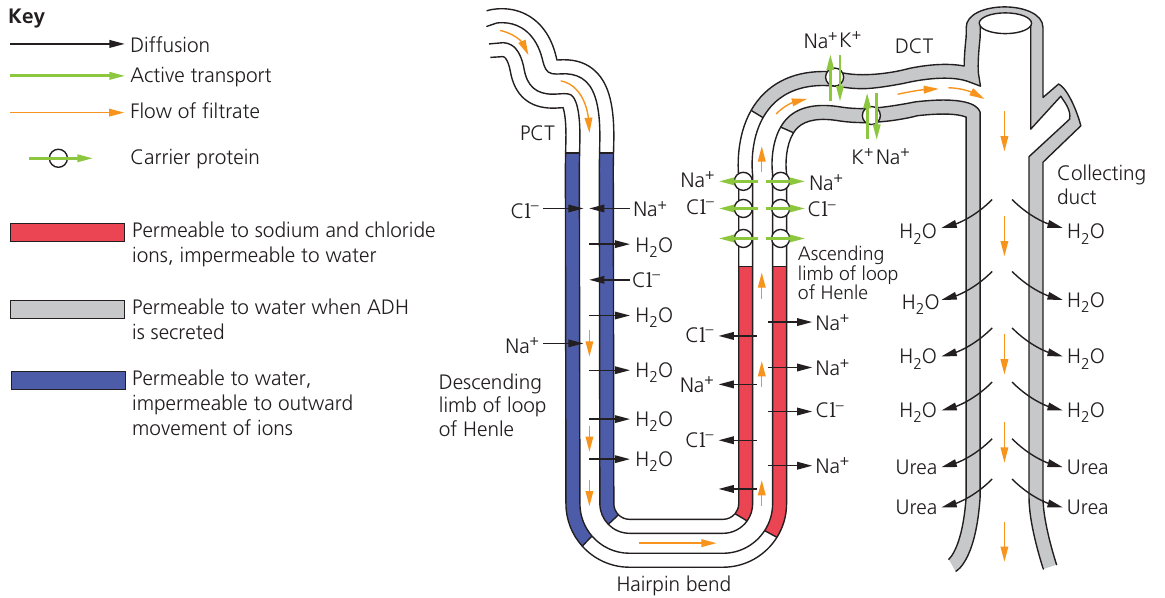
Function of the descending limb
As filtrate flows down the descending limb:
- Water diffuses out into surrounding tissue fluid by osmosis (the membrane is permeable to water)
- The membrane is impermeable to the outward movement of ions and urea
- Sodium and chloride ions diffuse into the filtrate from the surrounding tissue
- Filtrate becomes progressively more concentrated as it approaches the hairpin bend
Function of the ascending limb
As filtrate flows up the ascending limb:
- The membrane is impermeable to water, preventing water loss
- Sodium and chloride ions diffuse out into tissue fluid in the thin region
- In the thick region, cells rich in mitochondria actively pump and out of the filtrate
- Filtrate becomes progressively more dilute as ions are removed
- This active transport is the primary mechanism creating the low water potential in medullary tissue fluid
Countercurrent exchange mechanism
The parallel arrangement of loop limbs, vasa recta capillaries, and collecting ducts creates a countercurrent exchange system that maintains the concentration gradient:
- Descending capillaries lose water and gain sodium and chloride ions as blood flows into the medulla
- Ascending capillaries gain water and lose ions as blood flows back to the cortex
- Blood flows very slowly through vasa recta, minimising ion loss from medullary tissue
- Without this arrangement, blood would remove the concentrated ions, destroying the medulla's concentrating effect
Mammals with relatively long loops can generate much lower water potentials in their medulla than those with short loops, allowing greater urine concentration.
The Countercurrent Multiplier Effect
The countercurrent arrangement is crucial for maintaining the medullary concentration gradient. If the vasa recta ran parallel in the same direction as the loop of Henle, they would quickly wash away the ions being pumped out, preventing the concentration gradient from building up. The slow blood flow and countercurrent design preserve this gradient, which is essential for producing concentrated urine when water must be conserved.
Regulation of water content of the blood
The hypothalamus serves as the control centre for osmoregulation, containing osmoreceptors that detect changes in blood water potential. This is another example of homeostasis by negative feedback.
The role of ADH
When the body becomes dehydrated:
- Water loss (through sweating, breathing, reduced intake) makes blood plasma more concentrated
- Blood water potential decreases
- Osmoreceptors in the hypothalamus detect this change
- The hypothalamus stimulates thirst and drinking behaviour
- Neurosecretory neurones release ADH (antidiuretic hormone) from the posterior pituitary gland into the blood
- ADH travels to target cells in the DCT and collecting ducts
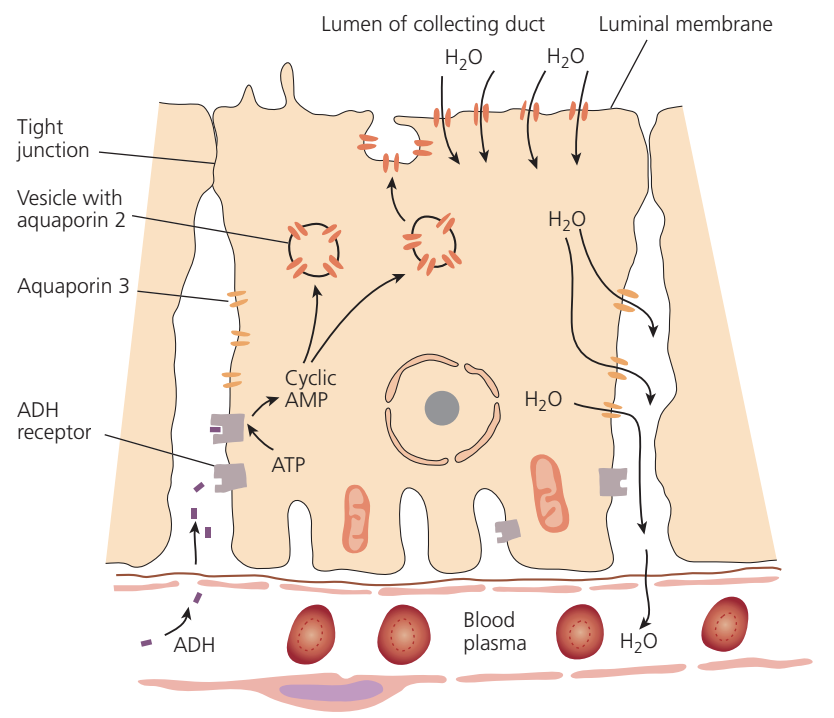
ADH mechanism at the cellular level
When ADH binds to receptors on collecting duct cells:
- The hormone-receptor complex activates adenylyl cyclase enzyme
- ATP is converted to cyclic AMP (cAMP), a second messenger
- cAMP triggers vesicles containing aquaporin 2 water channels to move to the luminal membrane
- Vesicles fuse with the membrane by exocytosis, inserting aquaporins
- Each aquaporin allows approximately water molecules per second to pass through
- Water moves by osmosis from urine into the concentrated medullary tissue fluid
- Water then enters blood capillaries for return to circulation
Aquaporin 3 channels permanently present in basal membranes allow water to exit cells into tissue fluid. ADH also increases permeability of cells at the collecting duct base to urea, allowing it to diffuse into medullary tissue fluid, further lowering water potential.
The Second Messenger System
ADH uses a second messenger system (cAMP) rather than entering cells directly. This is because ADH is a peptide hormone that cannot cross the cell membrane. The cAMP cascade amplifies the signal, allowing a small amount of ADH to trigger the insertion of many thousands of aquaporin channels.
When water is plentiful
When blood water potential is higher than the set point:
- Osmoreceptors are not stimulated
- ADH secretion stops
- Aquaporins are removed from luminal membranes by endocytosis
- Collecting duct walls become impermeable to water
- No water reabsorption occurs
- Large volumes of dilute urine are produced
This is a classic example of negative feedback regulation. When water levels are low, ADH is released to conserve water. When water levels return to normal, ADH secretion stops. This maintains blood water potential within a narrow range, preventing both dehydration and overhydration.
Control of ion excretion
The DCT determines the quantity of remaining ions excreted in urine. Sodium is the major ion in extracellular fluids (blood plasma and tissue fluid), and its concentration is carefully monitored by receptors in major arteries.
The role of aldosterone
When sodium levels are low, or when the body is dehydrated or has lost blood:
- The hormone aldosterone is secreted by the adrenal cortex
- This steroid hormone enters DCT cells and binds to receptors
- The hormone-receptor complex acts as a transcription factor
- Genes for carrier proteins are switched on
- More antiport carrier proteins are synthesised
- These carriers pump sodium ions out of filtrate and potassium ions into filtrate
- Sodium is conserved while excess potassium is excreted
These antiport carriers work similarly to those in nerve cells, transporting substances in opposite directions across membranes.
Aldosterone is a steroid hormone, unlike ADH which is a peptide. This means aldosterone can pass through cell membranes and directly affect gene transcription. The response is slower than ADH (hours vs. minutes) but produces longer-lasting changes in sodium handling.
Summary of kidney regions and functions
| Region | Structural features | Function |
|---|---|---|
| Capsule | Thin connective tissue layer with collagen fibres | Protection of kidney tissue |
| Cortex | Contains glomeruli, PCT, DCT, and blood vessels | Ultrafiltration in glomeruli; selective reabsorption in tubules |
| Medulla | Loops of Henle and collecting ducts with vasa recta capillaries | Creation of low water potential tissue fluid; water reabsorption from urine when ADH present |
| Pelvis | Urine-filled space with white fibrous tissue connecting to ureter | Collection of urine from collecting ducts |
| Ureter | Thick-walled tube with smooth muscle | Transport of urine to bladder by peristalsis |
Key Points to Remember:
- Nephrons are the functional units of the kidney - each filters blood, reabsorbs useful substances, and produces urine
- Ultrafiltration depends on structure: fenestrated endothelium with pores, basement membrane acting as a molecular sieve, and podocytes with slit pores between foot processes
- Selective reabsorption in the PCT uses indirect active transport: pumps create a sodium gradient that drives symport of glucose and amino acids
- The loop of Henle creates a water potential gradient through active transport of and in the thick ascending limb - this is maintained by countercurrent exchange
- ADH controls water reabsorption by inserting aquaporin water channels into collecting duct cell membranes, allowing osmotic water recovery when the body is dehydrated
- Aldosterone regulates sodium balance by increasing synthesis of antiport carriers in the DCT, conserving sodium while excreting excess potassium