Control of Blood Glucose Concentration and Diabetes (OCR A-Level Biology A): Revision Notes
Control of Blood Glucose Concentration and Diabetes
Blood glucose regulation
Glucose serves as the primary substrate for cellular respiration, providing essential energy for all tissues. However, glucose concentration must be carefully regulated because excessive levels disrupt water potential and osmosis across cell membranes. In severe cases, hyperglycaemia (abnormally high blood glucose) can be fatal.
In healthy individuals, blood glucose concentration fluctuates but remains within a tightly controlled range of . This narrow range is maintained through precise hormonal control mechanisms.
Factors increasing blood glucose concentration
Blood glucose levels rise through three main processes:
- Absorption of carbohydrate digestion products from the gut into the bloodstream
- Glycogenolysis — breakdown of glycogen stores in the liver to release glucose
- Gluconeogenesis — synthesis of glucose from non-carbohydrate molecules including lactate, amino acids, glycerol and fatty acids
Factors decreasing blood glucose concentration
Blood glucose levels fall through:
- Cellular uptake of glucose for respiration (particularly during exercise)
- Glycogenesis — conversion of glucose to glycogen for storage in the liver
- Conversion of glucose into lipids for long-term energy storage
Memory Aid:
- Genesis = creation → Glycogenesis creates glycogen
- Lysis = breakdown → Glycogenolysis breaks down glycogen
- Neo = new → Gluconeogenesis creates new glucose
Hormonal control
Two pancreatic hormones regulate blood glucose through antagonistic actions:
- Insulin lowers blood glucose concentration
- Glucagon raises blood glucose concentration
Insulin secretion and action
Beta cell structure and function
Beta cells within the islets of Langerhans act as both glucose sensors and insulin producers. At rest, the beta cell membrane maintains a potential difference through selective ion channel activity.
The resting state features:
- Open potassium channels allowing ions to diffuse out
- Closed calcium channels preventing entry
- Net negative charge inside the cell relative to outside
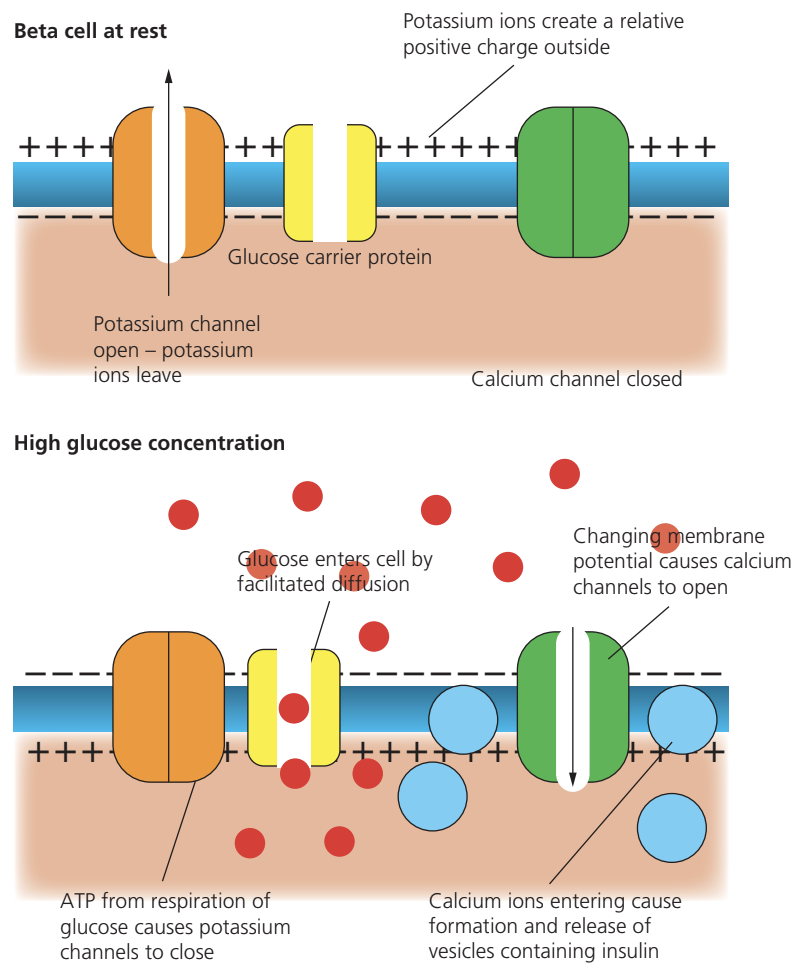
Mechanism of insulin release
When blood glucose concentration rises, the following sequence occurs:
- Glucose enters beta cells by facilitated diffusion through glucose carrier proteins
- Cellular respiration of glucose generates ATP
- High ATP concentration causes potassium channels to close
- Changing membrane potential triggers voltage-gated calcium channels to open
- Calcium influx stimulates vesicles containing insulin to fuse with the cell membrane
- Insulin is released by exocytosis into the bloodstream
Critical Mechanism: The ATP-sensitive potassium channels are the key glucose sensors in beta cells. When glucose levels rise, increased ATP production closes these channels, triggering the cascade that leads to insulin release.
Actions of insulin on target tissues
Insulin binds to specific receptors on muscle and liver cell membranes, triggering multiple responses:
- Increased membrane permeability to glucose, enhancing uptake by facilitated diffusion
- Activation of enzymes catalysing glycogenesis (glucose → glycogen conversion)
- Stimulation of increased respiration rate, particularly in muscle cells
- Promotion of glucose conversion into proteins and lipids
The liver stores the largest glycogen reserves, though muscle cells also maintain significant glycogen deposits. This distributed storage system allows for both rapid local energy release (in muscles) and sustained blood glucose regulation (from liver).
Negative feedback control of insulin
Insulin secretion operates through negative feedback:
- Rising blood glucose stimulates beta cells to release insulin
- Insulin causes blood glucose levels to fall through multiple mechanisms
- Falling glucose concentration reduces stimulus for insulin secretion
- Normal blood glucose concentration is restored
- Beta cells reduce insulin production
This prevents excessive glucose reduction below the normal range.
Glucagon secretion and action
Alpha cell function
Alpha cells in the pancreatic islets of Langerhans detect falling blood glucose and respond by secreting glucagon. This hormone exerts antagonistic effects to insulin.
Actions of glucagon
Glucagon raises blood glucose through two main mechanisms:
- Promoting glycogenolysis (glycogen → glucose conversion in the liver)
- Stimulating gluconeogenesis (synthesis of glucose from non-carbohydrate sources)
Memory Aid: GLUCAgon raises GLUCose — the similarity in names helps remember the function!
Negative feedback control of glucagon
Similar to insulin, glucagon operates through negative feedback:
- Falling blood glucose stimulates alpha cells to release glucagon
- Glucagon causes blood glucose to rise
- Rising glucose concentration reduces stimulus for glucagon secretion
- Normal blood glucose is restored
- Alpha cells reduce glucagon production
Diabetes mellitus
Diabetes mellitus is a chronic condition (lasting longer than three months) characterised by persistently elevated blood glucose concentration. Two distinct types exist with different underlying causes.
Type 1 diabetes (insulin-dependent)
Type 1 represents the less common form, typically diagnosed during childhood or early adulthood.
Cause: An autoimmune response destroys pancreatic beta cells, eliminating insulin production capability.
Pathology: Without insulin, blood glucose reaches dangerously high concentrations after eating (hyperglycaemia). The kidneys cannot reabsorb all filtered glucose, causing glucose to appear in urine.
Symptoms:
- Frequent urination (due to glucose in urine)
- Extreme tiredness (cells cannot absorb glucose for respiration)
- Excessive hunger
- Significant weight loss (carbohydrates provide no usable energy)
Critical Warning: Type 1 diabetes is fatal without treatment. The inability to utilize glucose for cellular respiration means cells cannot obtain energy from carbohydrates, leading to rapid deterioration.
Aetiology: The exact trigger remains uncertain, though potential factors include genetic predisposition and viral infections that provoke immune system overreaction.
Type 2 diabetes (non-insulin-dependent)
Type 2 accounts for approximately 90% of diabetes cases, most commonly developing during middle age.
Cause: Body cells become insensitive to insulin; insulin production may also decline. This results from combined genetic and lifestyle factors.
Risk factors:
- Obesity
- High blood cholesterol
- Elevated blood pressure
- Physical inactivity
- Genetic predisposition (certain ethnic groups show higher risk)
- Family history of type 2 diabetes
Symptoms: Similar to type 1 but developing gradually over years, contrasting with the rapid onset of type 1.
Treatment: Typically managed through low-sugar diet and medication (tablets), though insulin injections may be required in some cases.
Key Difference: Type 1 develops rapidly and occurs in childhood/early adulthood, while Type 2 develops gradually and typically appears in middle age. Type 1 requires insulin injections from diagnosis, while Type 2 can often be managed initially with diet and medication.
Research evidence: soft drinks and type 2 diabetes
A large-scale European study (1991-2007) investigated links between soft drink consumption and type 2 diabetes risk among 330,234 participants.
Research Study: Soft Drinks and Type 2 Diabetes Risk
The research compared three beverage types:
- Sugar-sweetened soft drinks
- Artificially sweetened soft drinks
- Fruit juices
Results expressed risk as hazard ratio (HR), where HR = 1.0 indicates no increased risk and HR = 2.0 indicates double the risk.
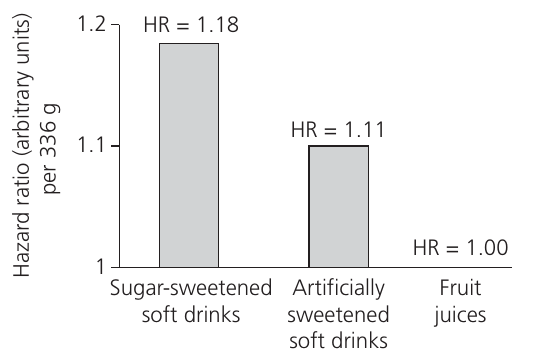
Findings per 336g serving:
- Sugar-sweetened soft drinks: HR = 1.18 (statistically significant increased risk)
- Artificially sweetened soft drinks: HR = 1.11 (not statistically significant)
- Fruit juices: HR = 1.00 (baseline, no increased risk)
Conclusion: Regular consumption of sugar-sweetened soft drinks increases type 2 diabetes risk, whilst fruit juices show no such association.
Treatment and management
Producing insulin
Historically, people with diabetes relied on insulin extracted from pig and cattle pancreases. Though effective, animal insulin differs slightly from human insulin at the molecular level, requiring higher dosages and sometimes causing localised injection site reactions.
Genetically modified insulin production
Modern treatment uses human insulin produced by genetically modified bacteria or yeasts. Genetic engineering techniques enable insertion of the human insulin gene into bacterial plasmids (circular DNA molecules capable of independent replication). When the plasmid enters bacteria, cell division produces colonies all secreting human insulin.
Advantages of GM human insulin:
- Identical to naturally produced human insulin, minimising immune responses
- Works more efficiently than animal insulin, requiring lower doses
- Production independent of animal pancreas supply
- Demand-responsive manufacturing capacity
- Acceptable to religious groups and animal welfare advocates
- Lower production costs compared to animal extraction
- Zero infection risk from viruses or prions
Future treatments: stem cell therapy
Stem cells are undifferentiated cells capable of developing into any cell type. Current research explores treating stem cells to differentiate into pancreatic beta cells for transplantation.
Successful transplantation would:
- Replace destroyed beta cells
- Enable natural insulin production
- Potentially cure type 1 diabetes
Current Limitations: Whilst experiments in mice show promise, the research remains at early stages. Widespread clinical application likely requires several more years. Additionally, stem cell therapy would not benefit many type 2 diabetes cases, where beta cells remain intact but target tissues show insulin insensitivity.
Glucose tolerance testing
Glucose tolerance tests help diagnose type 1 diabetes by measuring blood glucose response to a standard glucose load.
Glucose Tolerance Test Procedure:
Method:
- Patient fasts (water only) for 12 hours
- Patient consumes glucose drink (50g in 200cm³)
- Blood glucose monitored every 30 minutes for 3 hours
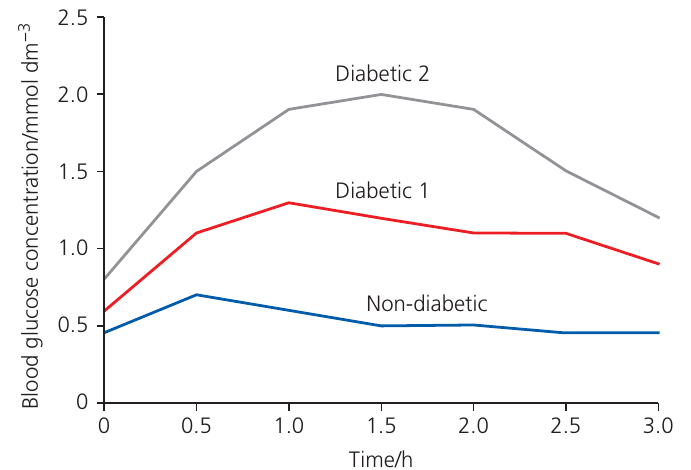
Interpretation:
- Non-diabetic: Blood glucose rises moderately then returns rapidly to baseline
- Diabetic: Blood glucose shows excessive rise and slow return to baseline
- Severity variation: Degree of abnormal response correlates with disease severity
Different baseline glucose concentrations before testing may reflect varying glycogen stores, recent physical activity, or (in diabetic patients) previous blood glucose levels.
Remember!
Key Points to Remember:
-
Blood glucose is maintained between through antagonistic actions of insulin and glucagon, both operating via negative feedback loops
-
Insulin (from beta cells) lowers glucose by promoting cellular uptake, glycogenesis, and increased respiration; glucagon (from alpha cells) raises glucose through glycogenolysis and gluconeogenesis
-
Type 1 diabetes results from autoimmune destruction of beta cells, requiring lifelong insulin injections; type 2 diabetes involves insulin insensitivity linked to genetic and lifestyle factors
-
Genetically modified bacteria produce human insulin more safely, effectively and ethically than historical animal sources
-
High sugar-sweetened soft drink consumption correlates with increased type 2 diabetes risk, whilst fruit juice consumption shows no such association