Urine Tests and Kidney Failure (OCR A-Level Biology A): Revision Notes
Urine Tests and Kidney Failure
Urine analysis in medical diagnosis
Urine samples provide valuable diagnostic information about kidney function and metabolic disorders. Medical professionals commonly request urine samples during examinations to test for various substances that should not normally be present, or to check concentrations of substances that should be regulated.
Urine analysis is a non-invasive diagnostic tool that can reveal information about kidney function, metabolic disorders, infections, and even pregnancy. The substances present in urine—or their concentrations—can indicate specific physiological problems before other symptoms become apparent.
Glucose detection in urine
Under normal physiological conditions, the proximal convoluted tubule (PCT) reabsorbs all glucose from the filtrate back into the bloodstream. However, when blood glucose concentration exceeds a critical level called the renal threshold ( blood), the PCT cells cannot reabsorb all the glucose molecules, resulting in glucose appearing in urine.
The detection of glucose in urine often signals problems with glucose homeostatic control, particularly involving insulin function. This can indicate diabetes mellitus, where the body either does not produce sufficient insulin or cells do not respond properly to insulin.
The presence of glucose in urine is NOT normal and typically indicates that blood glucose levels have exceeded the renal threshold. This is one of the key diagnostic indicators for diabetes mellitus and requires immediate medical attention.
Protein detection in urine
Serum albumin (also called albumen) represents the most abundant plasma protein with a relative molecular mass (RMM) of . Since most plasma proteins have RMM values greater than , they should not normally pass through the filtration membrane in the glomerulus.
Albumin's negative charge means only minimal quantities undergo filtration. Any albumin that does pass into the filtrate gets reabsorbed by endocytosis in the PCT, where it undergoes breakdown and the resulting amino acids return to the bloodstream.
The large size and negative charge of albumin molecules create a double barrier against filtration. The filtration membrane's pores are too small for most large proteins, and the negative charge on the basement membrane repels negatively charged proteins like albumin.
When protein appears in urine, it can suggest several conditions:
- Elevated blood pressure damaging filtration membranes
- Kidney infection affecting normal function
- Malfunction of the filtration mechanism
- Pregnancy (though this typically resolves after delivery)
Common Mistake: Students often assume all proteins in blood are filtered and then reabsorbed. In reality, most plasma proteins should never enter the filtrate because they are too large to pass through the glomerular filtration membrane. Their presence in urine indicates membrane damage or dysfunction.
Ketone detection in urine
People with diabetes produce ketones during metabolism. The presence of ketones—specifically acetone (propanone) and acetoacetate—in blood and urine serves as an indicator of diabetes mellitus. These compounds form when the body cannot use glucose effectively and instead breaks down fats for energy.
Nitrite ion testing
Positive results for nitrite ions in urine indicate bacterial infection in the urinary tract. Bacteria convert nitrates naturally present in urine into nitrites, making this a useful diagnostic marker.
Multi-factor urinalysis strips
Rather than testing for individual substances separately, modern urinalysis test strips can simultaneously test for ten different factors, including:
- Glucose
- Protein
- Ketones
- Nitrite ions
- pH level
- Other diagnostic markers
These strips contain specific chemicals that react with target substances, producing colour changes to indicate positive results.

Multi-factor test strips provide a rapid screening tool that allows healthcare professionals to check multiple parameters in seconds. This efficiency makes them ideal for routine examinations and emergency assessments, though positive results often require confirmation through more specific laboratory tests.
Pregnancy testing
Pregnancy tests detect the hormone human chorionic gonadotrophin (hCG), which the early embryo secretes shortly after implantation in the uterus. These tests use monoclonal antibodies—identical antibodies produced by a single clone of B lymphocytes, all specific to hCG. Using monoclonal antibodies reduces false results because all antibodies have identical binding properties.

How pregnancy tests work
Pregnancy tests employ a sophisticated two-zone system based on antibody-antigen interactions:
Understanding the Two-Zone System:
The pregnancy test uses two distinct detection zones to provide both a test result and quality control:
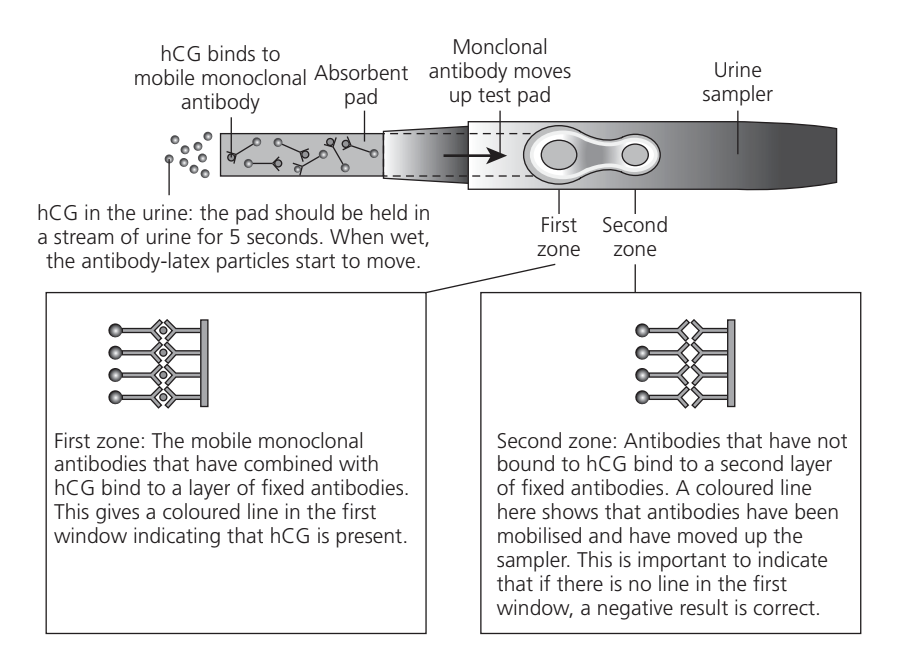
First zone (test line): When urine containing hCG contacts the test pad, mobile monoclonal antibodies bind to hCG molecules. As the liquid moves up the strip by capillary action, these antibody-hCG complexes reach the first zone where fixed antibodies capture them. This binding produces a coloured line, confirming hCG presence and indicating pregnancy.
Second zone (control line): Antibodies that have not bound to hCG continue moving up the strip and bind to a second layer of fixed antibodies. This creates a coloured control line that confirms the test is functioning correctly. If no line appears in the first window but a line appears in the second window, this indicates a genuine negative result rather than a faulty test.
The test requires holding the absorbent pad in a urine stream for approximately five seconds. When wet, antibody-latex particles mobilize and begin moving through the test system.
The use of monoclonal antibodies is crucial for test accuracy. Because all antibodies come from a single clone of B lymphocytes, they are identical in structure and have the same binding specificity for hCG. This uniformity minimizes false positives that could occur with polyclonal antibodies (which have varying specificities).
Anabolic steroid testing in athletes
Athletes undergo regular testing to detect anabolic steroids, which some use to increase muscle mass. These substances work by stimulating protein synthesis.
Testing laboratories use gas chromatography or mass spectrometry to detect anabolic steroids in urine. Since these drugs are based on steroid hormones and may have a half-life of approximately hours, timing of sample collection is important. The half-life represents the time required for a drug's blood concentration to decrease to half its initial value.
The concept of half-life is critical in drug testing. After hours, only 50% of the original steroid concentration remains in the blood. After hours ( half-lives), only 25% remains. This exponential decay means that strategic timing of tests is necessary to detect substances before they fall below detectable levels.
Kidney failure
Causes of kidney dysfunction
Kidneys may fail due to various factors:
- Blood loss during accidents
- Chronic high blood pressure
- Diabetes complications
- Overuse of certain medications (such as aspirin)
- Infections
Consequences of kidney failure
When kidneys fail, the condition can prove fatal within a short timeframe because urea, water, salts and toxins accumulate rather than being excreted. The glomerular filtration rate (GFR) decreases, and levels below represent a dangerous threshold.
Critical Threshold: A GFR below indicates serious kidney dysfunction requiring immediate medical intervention. At this level, the kidneys cannot adequately filter waste products from the blood, leading to potentially life-threatening complications.
Kidney failure prevents maintenance of proper ion concentrations and charged compound levels in the blood, leading to serious complications.
Potassium ion accumulation causes:
- Abdominal cramping
- Tiredness
- Muscle weakness and paralysis
- Slowed impulses from the sinoatrial node
- Cardiac arrhythmia
- Potential cardiac arrest
Sodium imbalance affects:
- Fluid balance
- Neuromuscular function
- Acid-base balance
When kidneys cannot excrete sodium properly, patients may experience:
- Disorientation
- Muscle twitches
- Elevated blood pressure
- General weakness
Why Ion Balance is Critical:
Potassium ions are particularly dangerous when elevated because they affect the heart's electrical activity. The sinoatrial node, which sets the heart's rhythm, becomes less responsive, potentially leading to cardiac arrhythmia or arrest.
Sodium ions regulate osmotic balance and nerve impulse transmission. Imbalances disrupt fluid distribution between cells and extracellular fluid, affecting blood pressure and cellular function.
Kidney failure can occur suddenly and last briefly (acute failure) or develop as a long-term condition (chronic failure).
Treatment options for kidney failure
Two main approaches treat kidney failure:
- Dialysis - removes toxins, metabolic wastes and excess substances through diffusion across dialysis membranes
- Kidney transplantation - provides a permanent replacement organ
Haemodialysis
Dialysis means separating small and large molecules using a partially permeable membrane. Haemodialysis involves regular treatment sessions, either at hospital or at home.
Haemodialysis mechanism
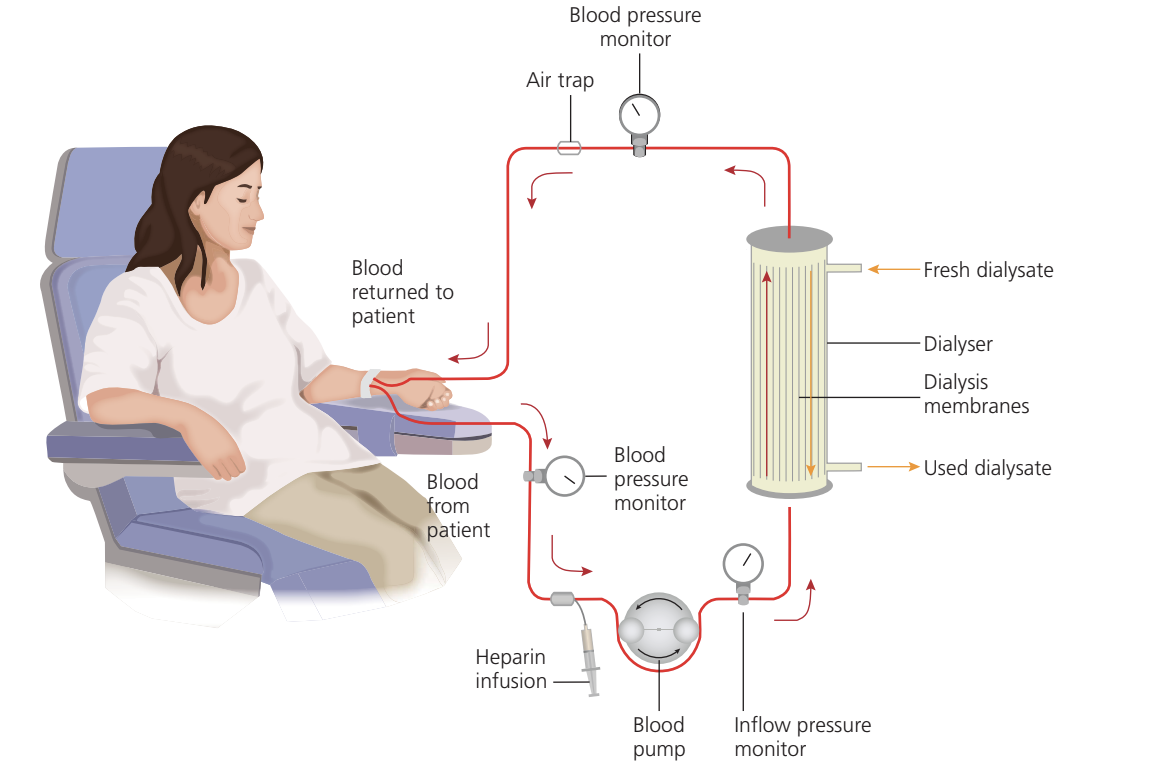
In the haemodialyser, partially permeable dialysis membranes separate blood from dialysate (dialysis fluid). Blood flows through tubes made of dialysis membrane, with dialysate surrounding these tubes.
The dialysate contains required blood substances (such as glucose and sodium ions) at physiologically correct concentrations. Importantly, dialysate contains no urea, creating a concentration gradient that drives urea diffusion from blood into dialysate, which then goes to waste.
Counter-current Flow Principle:
Counter-current flow represents a key design feature—dialysate and blood flow in opposite directions. This arrangement maintains a concentration gradient along the entire length of the dialyser, maximizing efficiency of waste removal.
If blood and dialysate flowed in the same direction, equilibrium would be reached partway through the dialyser, reducing overall efficiency. Counter-current flow ensures that fresh dialysate always encounters blood with higher urea concentrations, maintaining the driving force for diffusion throughout the system.
Each passage of blood through the dialysis machine removes some urea. After approximately three hours of treatment, nearly all urea has been removed from the blood.
During treatment, heparin is added to blood to prevent clotting within the tubing system.

Dialysate composition
Dialysate must contain:
- Glucose at normal blood concentration
- Sodium ions at physiological levels
- Other essential ions at appropriate concentrations
- No urea (to establish diffusion gradient)
- No other metabolic wastes
The dialysate composition is carefully controlled to match normal blood plasma for substances that should be retained in the blood. By having glucose and essential ions at normal concentrations, there is no net diffusion of these substances. Only waste products like urea, which are absent from dialysate, diffuse out of the blood.
Peritoneal dialysis
The alternative form of dialysis uses the patient's own peritoneum as the dialysis membrane. Medical staff insert dialysate through a catheter into the abdominal cavity. Urea, other metabolic wastes and excess substances diffuse from blood across the peritoneum (the lining of the abdomen) into the dialysate. After a suitable period, the dialysate is drained and replaced with fresh fluid.
Peritoneal dialysis offers greater flexibility than haemodialysis as it can be performed at home and doesn't require connection to a dialysis machine. However, it requires multiple fluid exchanges daily and carries a risk of peritoneal infection.
Kidney transplantation
Dialysis places severe restrictions on patients' lives, including:
- Regular hospital or clinic visits for treatment
- Carefully controlled diet to limit urea production
- Salt intake restrictions
Kidney transplantation offers a solution to these limitations. Only one functioning kidney is required for normal life, but finding suitable donors presents challenges.
Transplant requirements
Successful transplantation requires:
- Compatible blood groups between donor and recipient
- Tissue matching (especially important for organs from deceased donors)
- Less stringent matching requirements for living donor kidneys
Transplant considerations
Transplantation involves several risks:
- Standard surgical operation risks
- Immune rejection of the transplanted organ
- Side effects from immunosuppressive drugs
Immunosuppression is Mandatory:
Transplant recipients must take immunosuppressive drugs indefinitely to prevent their immune system rejecting the donor kidney, which usually has a different tissue type. These medications carry their own risks and side effects but are necessary for transplant success.
Stopping immunosuppressive medication can lead to rapid rejection of the transplanted organ, requiring return to dialysis or emergency re-transplantation.
Key Points to Remember:
-
The renal threshold ( blood) determines when glucose appears in urine—exceeding this level may indicate diabetes.
-
Protein in urine signals kidney damage, high blood pressure or infection, since albumin (RMM ) should not normally pass through filtration membranes.
-
Pregnancy tests use monoclonal antibodies specific to hCG in a two-zone system: the test line detects pregnancy, while the control line confirms the test is working.
-
Haemodialysis removes urea by diffusion across dialysis membranes, with blood and dialysate flowing in opposite directions (counter-current) to maintain concentration gradients throughout the dialyser.
-
Kidney failure below GFR of causes dangerous accumulation of potassium ions (leading to cardiac problems) and sodium ions (affecting fluid balance and neuromuscular function).
-
Dialysate must contain glucose and essential ions at normal blood concentrations but no urea or metabolic wastes to establish the concentration gradients needed for waste removal.
-
Kidney transplantation provides a permanent solution but requires lifelong immunosuppressive medication to prevent organ rejection.