Hormones and the Pancreas (OCR A-Level Biology A): Revision Notes
Hormones and the Pancreas
Introduction to pancreatic hormones
The pancreas plays a critical role in maintaining stable blood glucose concentrations through hormone secretion. Unlike the nervous system, which provides rapid, short-term control over specific organs, hormonal regulation offers sustained control over minutes, hours, or even years. Hormones travel via the bloodstream, reaching all tissues but affecting only those with specific receptors.
Hormonal vs Nervous Control: While the nervous system provides rapid, precise, and short-lived responses to specific organs, the endocrine system through hormones offers slower but more sustained control that can last from minutes to years. This makes hormonal regulation ideal for long-term processes like metabolism and growth.
Structure and function of the pancreas
Location and dual role
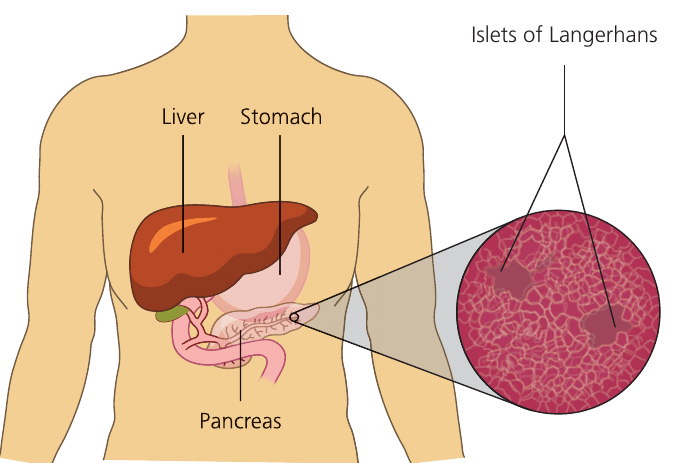
The pancreas sits in the abdominal cavity, positioned near the stomach and liver. This organ performs two distinct functions, operating as both an endocrine gland and an exocrine gland.
An endocrine gland secretes hormones directly into the bloodstream without using ducts. In contrast, an exocrine gland releases substances through ducts. The pancreas demonstrates both capabilities: its exocrine tissue produces pancreatic juice containing digestive enzymes, which travels via the pancreatic duct to the small intestine. Meanwhile, its endocrine tissue secretes hormones straight into the blood.
Understanding the Terminology: The terms "endocrine" and "exocrine" help distinguish between secretion methods:
- Endo- means "within" – hormones go directly into the blood
- Exo- means "outside" – substances are secreted through ducts to external environments (like the digestive tract)
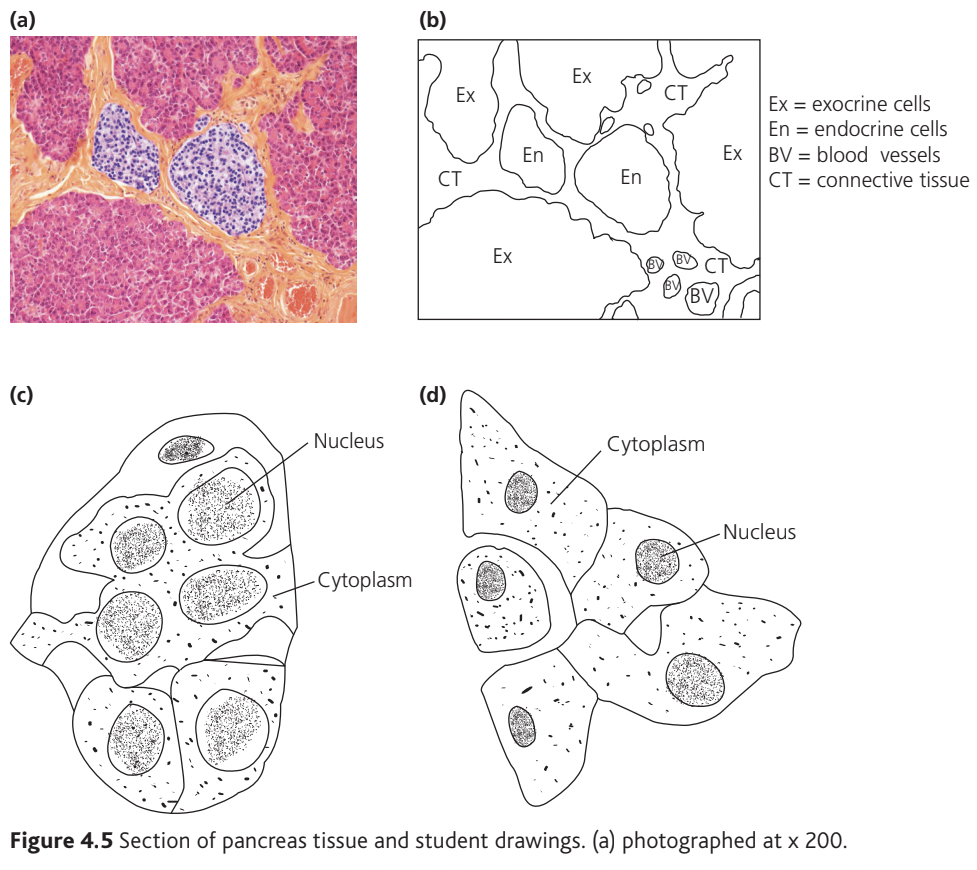
Microscopic structure
When examined under a microscope, pancreatic tissue reveals these two functional regions clearly. The majority of pancreatic cells form the exocrine tissue, appearing as clusters of enzyme-secreting cells. Scattered throughout this exocrine tissue are small, distinct groups of cells called the islets of Langerhans, which constitute the endocrine tissue.
The islets of Langerhans
The islets of Langerhans contain two principal cell types:
Alpha cells (α-cells):
- Larger in size but less numerous
- Secrete the hormone glucagon
- Raise blood glucose concentration
Beta cells (β-cells):
- Smaller in size but more abundant
- Secrete the hormone insulin
- Lower blood glucose concentration
Both cell types are intimately associated with blood vessels, allowing rapid hormone secretion into the circulation.
Key Cell Distinction: Remember the opposing roles: Alpha cells produce glucagon (raises glucose), while Beta cells produce insulin (lowers glucose). Despite alpha cells being larger, beta cells are more numerous in the islets. Both are closely associated with blood capillaries for immediate hormone release.
Blood glucose regulation
The importance of glucose control
Glucose serves as the primary respiratory substrate, providing energy for cellular processes. All tissues require a constant glucose supply to function properly. However, maintaining blood glucose within a specific range is essential for two reasons:
- Energy availability – cells need sufficient glucose for respiration
- Osmotic balance – excessive glucose concentration disrupts water potential, affecting osmosis across cell membranes
In healthy individuals, blood glucose concentration remains between mmol dm⁻³ and mmol dm⁻³. Values outside this range can impair body function, with very high concentrations potentially proving fatal, as seen in uncontrolled diabetes.
Critical Range: The normal blood glucose range of - mmol dm⁻³ must be maintained for two vital reasons:
- Too low = insufficient energy for cellular respiration
- Too high = disrupts osmotic balance and water potential in cells
Severe deviations from this range can be life-threatening.
Factors increasing blood glucose
Three processes elevate blood glucose concentration:
- Carbohydrate digestion – absorption of glucose and other monosaccharides from the small intestine following digestion
- Glycogenolysis – the breakdown of glycogen stores in the liver, releasing glucose into the bloodstream
- Gluconeogenesis – synthesis of new glucose from non-carbohydrate molecules including lactate, amino acids, glycerol, and fatty acids
Understanding the Terminology: Breaking down the word parts helps remember these processes:
- Glyco- relates to glycogen
- Gluco- relates to glucose
- -lysis means breakdown
- -genesis means creation/synthesis
- neo- means new
Therefore:
- Glycogenolysis = glycogen breakdown
- Glycogenesis = glycogen creation
- Gluconeogenesis = new glucose creation (from non-carbohydrate sources)
Factors decreasing blood glucose
Three processes reduce blood glucose concentration:
- Cellular respiration – glucose uptake by cells for ATP production, which increases during physical activity
- Glycogenesis – conversion of glucose to glycogen for storage in the liver and muscles
- Lipid synthesis – transformation of excess glucose into fat for long-term energy storage
Glycogenesis is the synthesis of glycogen from glucose, where 'genesis' indicates creation or synthesis.
Hormonal control mechanisms
Two pancreatic hormones maintain blood glucose homeostasis through opposing actions:
| Hormone | Source | Effect on blood glucose | Mechanisms |
|---|---|---|---|
| Insulin | Beta cells (β-cells) | Decreases | Promotes glycogenesis, increases glucose uptake by cells, stimulates lipid synthesis |
| Glucagon | Alpha cells (α-cells) | Increases | Promotes glycogenolysis and gluconeogenesis |
When blood glucose rises above mmol dm⁻³, beta cells detect this change and secrete insulin. Insulin binds to receptors on liver and muscle cells, triggering glucose uptake and conversion to glycogen (glycogenesis).
When blood glucose falls below mmol dm⁻³, alpha cells respond by secreting glucagon. Glucagon targets liver cells, stimulating glycogen breakdown (glycogenolysis) and glucose synthesis from other molecules (gluconeogenesis), releasing glucose into the blood.
How Blood Glucose Regulation Works:
Scenario 1: After a carbohydrate-rich meal
- Blood glucose rises above mmol dm⁻³
- Beta cells detect the increase
- Insulin is secreted into the bloodstream
- Liver and muscle cells respond by taking up glucose
- Glycogenesis occurs – glucose converted to glycogen
- Blood glucose returns to normal range
Scenario 2: During exercise or fasting
- Blood glucose falls below mmol dm⁻³
- Alpha cells detect the decrease
- Glucagon is secreted into the bloodstream
- Liver cells respond to the signal
- Glycogenolysis and gluconeogenesis occur
- Glucose released into blood
- Blood glucose returns to normal range
Memory Aid: Think of it this way:
- Insulin = IN (stores glucose in cells and glycogen)
- Glucagon = GO (glucose goes out from stores into blood)
Mode of action of hormones
First and second messengers
Hormonal signaling involves two types of messenger molecules. Understanding this mechanism is essential for appreciating how hormones produce specific effects despite traveling throughout the entire body.
The first messenger is the hormone itself, which travels in the bloodstream from its endocrine gland to target tissues. However, many hormones (including insulin and adrenaline) cannot cross the cell membrane due to their chemical nature. Instead, they bind to specific receptors on the cell surface.
The second messenger is an intracellular signaling molecule that transmits the hormone's signal inside the cell, triggering the appropriate cellular response. This two-messenger system allows hormones to affect specific cells while leaving others unaffected.
Why Two Messengers? Many hormones, including insulin, glucagon, and adrenaline, are hydrophilic (water-soluble) molecules that cannot pass through the lipid bilayer of cell membranes. The two-messenger system solves this problem:
- The hormone (first messenger) binds to surface receptors
- This triggers production of a second messenger inside the cell
- The second messenger activates the cellular response
This mechanism also allows for signal amplification – one hormone molecule can trigger production of many second messenger molecules, creating a powerful cellular response.
Example: Adrenaline signaling pathway
Although adrenaline comes from the adrenal glands (located above the kidneys) rather than the pancreas, it provides a clear example of the first and second messenger mechanism:
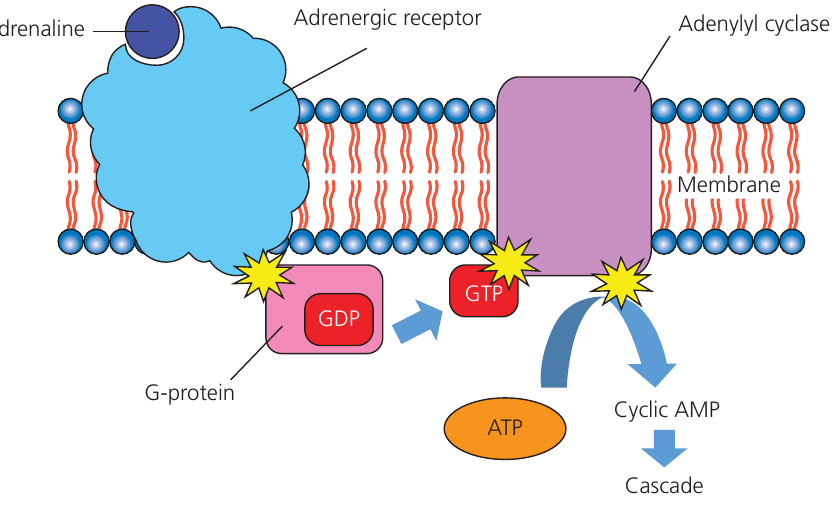
The signaling cascade proceeds through five stages:
- Receptor binding – adrenaline binds to a specific adrenergic receptor on the cell membrane
- G-protein activation – receptor binding activates a G-protein complex inside the cell, which contains guanosine diphosphate (GDP)
- GDP to GTP conversion – the GDP is converted to guanosine triphosphate (GTP), activating the G-protein
- Adenylyl cyclase activation – activated GTP stimulates the membrane enzyme adenylyl cyclase, which converts ATP to cyclic adenosine monophosphate (cyclic AMP or cAMP)
- Signal amplification – cAMP acts as the second messenger, initiating a cascade of reactions that produce the hormone's effects within the target cell
Signal Amplification: The beauty of this system lies in its amplification effect. A single adrenaline molecule binding to one receptor can activate multiple G-proteins. Each activated G-protein can activate one adenylyl cyclase enzyme. Each adenylyl cyclase can produce hundreds of cAMP molecules. Each cAMP molecule can trigger multiple downstream reactions.
This creates a cascade effect where one hormone molecule ultimately generates thousands of product molecules, producing a substantial cellular response from a tiny initial signal.
Importantly, adrenaline never enters the cell. The hormone binds externally, whilst cyclic AMP carries the message internally, triggering appropriate cellular responses. This mechanism allows signal amplification, where a single hormone molecule can generate thousands of second messenger molecules, producing a substantial cellular response.
Application to pancreatic hormones
Insulin and glucagon employ similar second messenger systems, though their specific pathways and effects differ. Both hormones bind to surface receptors on target cells, triggering intracellular cascades that ultimately alter glucose metabolism. This explains how these hormones can produce widespread but specific effects throughout the body – they travel everywhere via the blood, but only cells with the appropriate receptors will respond.
Insulin and Glucagon Signaling: While we've used adrenaline as an example, insulin and glucagon work through similar mechanisms:
- Both are first messengers that cannot cross cell membranes
- Both bind to specific receptors on target cells (mainly liver and muscle cells)
- Both trigger intracellular second messenger cascades
- The specific pathways and ultimate effects differ based on the hormone and target cell type
Remember!
Key Points to Remember:
-
The pancreas functions as both an endocrine gland (secreting insulin and glucagon into blood) and an exocrine gland (secreting digestive enzymes through ducts)
-
Islets of Langerhans contain alpha cells producing glucagon and beta cells producing insulin
-
Normal blood glucose concentration ranges from to mmol dm⁻³
-
Insulin lowers blood glucose by promoting glycogenesis and cellular glucose uptake, whilst glucagon raises blood glucose through glycogenolysis and gluconeogenesis
-
Hormones work via a first messenger (the hormone) and second messenger (e.g., cyclic AMP) system, allowing specific cellular responses despite hormones traveling throughout the body
-
Process terminology:
- Glycogenolysis = glycogen breakdown
- Glycogenesis = glycogen synthesis
- Gluconeogenesis = new glucose synthesis from non-carbohydrates
-
The two-messenger system allows for signal amplification, where one hormone molecule can trigger thousands of cellular responses